
What follows are excerpts from Dr. Farkas’ post PulmCrit- A better approach to Torsade de Pointes July 2, 2018:
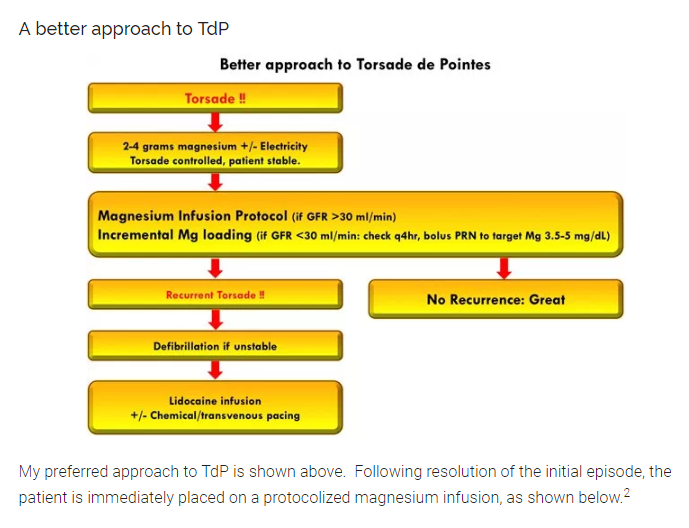
In his post, Dr. Farkas first reviews the standard approach to the treatment of Torsade de Pointes and explains why the standard approach can fail. And then Dr. Farkas proposes another approach:
The rationale for using a magnesium infusion is as follows:
- A magnesium infusion will maintain elevated magnesium levels for at least 24 hours. Like a naloxone infusion for methadone poisoning, this will allow magnesium to out-last other drugs that caused the TdP (e.g. dofetilide).
- Many patients with TdP have an intracellular magnesium deficiency (which can occur despite normal serum levels, since most magnesium is located intracellularly). Magnesium isn’t absorbed by cells very efficiently, so a couple grams of magnesium won’t replete the intracellular magnesium deficiency. However, a 24-hour exposure to elevated serum magnesium allows magnesium to eventually soak into the cardiomyocytes. Repletion of intracellular magnesium stores provides ongoing protection against TdP, even after the infusion is stopped and the patient leaves the ICU.
- A protocolized magnesium infusion is quite safe. Compared to the risk of recurrent arrhythmia and cardiac arrest from inadequately treated TdP, magnesium infusion is almost certainly the safer route to go.
The protocol should be included in the patient’s chart in a prominent location, so that everyone caring for the patient can literally be “on the same page.” This is essential to achieve continuation of the magnesium infusion. Without a well-defined protocol, high serum magnesium levels will provoke anxiety, causing the infusion to be shut off prematurely.
Some more detail about the magnesium infusion
The magnesium protocol shown above is based on clinical trials involving atrial fibrillation (in fact, it is more conservative than these studies, to establish a greater margin of safety). Thus, there is a literature base demonstrating that this is safe among sick ICU patients, in the absence of severe renal failure.3
Review all the information in Dr. Farkas’ section Some more detail about the magnesium infusion. This section has more information on Dr. Farkas’ protocol.



