
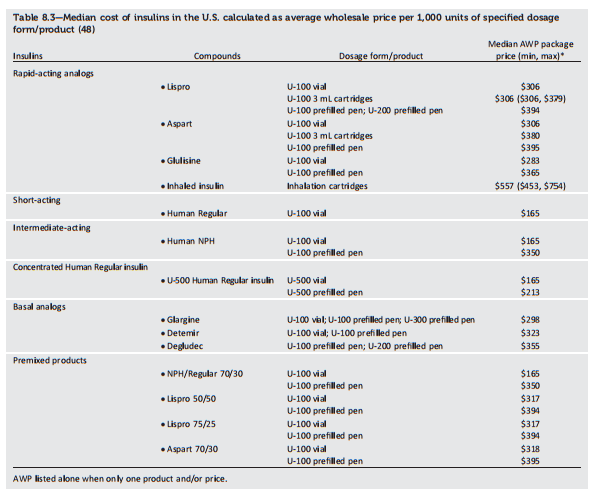
The following table is from p S72 of Resource (2)
The following text is from p S73 of Resource (2)
Combination Injectable Therapy
If basal insulin has been titrated to an acceptable fasting blood glucose level (or if the dose is .0.5 units/kg/day) and A1C remains above target, consider advancing to combination injectable therapy (Fig. 8.2). When initiating combination injectable therapy, metformin therapy should be maintained while other oral agents may be discontinued on an individual basis to avoid unnecessarily complex or costly regimens (i.e., adding a fourth antihyperglycemic agent). In general, GLP-1 receptor agonists should not be discontinued with the initiation of basal insulin. Sulfonylureas, DPP-4 inhibitors, and GLP-1 receptor agonists are typically stopped once more complex insulin regimens beyond basal are used. In patients with suboptimal blood glucose control, especially those requiring large insulin doses, adjunctive use of a thiazolidinedione or SGLT2 inhibitor may help to improve control and reduce the amount of insulin needed, though potential side effects should be considered. Once an insulin regimen is initiated, dose titration is important with adjustments made in both mealtime and basal insulins based on the blood glucose levels and an understanding of the pharmacodynamic profile of each formulation (pattern control).
Studies have demonstrated the noninferiority of basal insulin plus a single injection of rapid-acting insulin at the largest meal relative to basal insulin plus a GLP-1 receptor agonist relative to two daily injections of premixed insulins (Fig. 8.2). Basal insulin plus GLP-1 receptor agonists are associated with less hypoglycemia and with weight loss instead of weight gain but may be less tolerable and have a greater cost (37,38).
Please see the text continuation of the above on p S73 for more details on Combination Injectable Therapy.
Resources:
(1) CONSENSUS STATEMENT BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY ON THE COMPREHENSIVE TYPE 2 DIABETES MANAGEMENT ALGORITHM – 2017 EXECUTIVE SUMMARY [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Endocr Pract. 2017 Feb;23(2):207-238. doi: 10.4158/EP161682.CS. Epub 2017 Jan 17.
(2) AMERICAN DIABETES ASSOCIATION STANDARDS OF MEDICAL CARE IN DIABETES—2017 [Full Text PDF]. January 2017 Volume 40, Supplement 1.
(3) Patient-directed titration for achieving glycaemic goals using a once-daily basal insulin analogue: an assessment of two different fasting plasma glucose targets – the TITRATETM study [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Diabetes Obes Metab. 2009 Jun;11(6):623-31. doi: 10.1111/j.1463-1326.2009.01060.x.



