
Patients presenting to the emergency department with chest discomfort or other symptoms that are due to an ST elevation myocardial infarction, a non-ST segment elevation myocardial infarction, or unstable angina are said to have an acute coronary syndrome (ACS).
So how do we determine if the patient’s symptoms are likely due to an acute coronary syndrome?
The 2011 ACCF/AHA Focused Update Incorporated Into the ACC/AHA 2007 Guidelines for the Management of Patients With Unstable Angina/Non−ST-Elevation Myocardial Infarction gives the following guidance (Table 6, e441).
There is a high likelihood that the signs and symptoms represent an ACS due to coronary artery disease if any of the following are present:
A history of:
a. Chest or left arm pain or discomfort as chief symptom reproducing prior documented angina b. known history of coronary artery disease including myocardial infarction.
Examination showing: a. a transient mitral regurgitation murmur b. hypotension
c. diaphoresis d. pulmonary edema or rales
An ECG showing: a. new or presumably new ST-segment deviation (1 mm or greater) or T wave inversion in multiple precordial leads
Carding markers (blood tests) showing: a. an elevated troponin I, troponin T, or CK-MB
There is a intermediate likelihood that the signs and symptoms represent an ACS due to coronary artery disease if there are no high likelihood features above and there are the presence of any of the following:
A history of:
a. chest or left arm pain as the chief symptom
b. age greater than 70 years
c. male sex d. diabetes mellitus
Examination showing: a. extracardiac vascular disease
An ECG showing: a. fixed Q waves
b. ST depression of 0.5 to 1 mm or T wave inversion greater than 1 mm
Carding markers (blood tests) showing: a. normal troponin I, troponin T, or CK-MB
There is a low likelihood that the signs and symptoms represent an ACS due to coronary artery disease if there are no high likelihood features above and no intermediate likelihood features above but the patient may have:
A history of: a. probable ischemic symptoms in the absence of any of the intermediate likelihood characteristics
b. recent cocaine use
Examination showing: a. chest discomfort reproduced by palpation
An ECG showing: a. T wave flattening or inversion of less than 1 mm in leads with a dominant R wave b. Normal ECG
Carding markers (blood tests) showing: a. normal troponin I, troponin T, or CK-MB
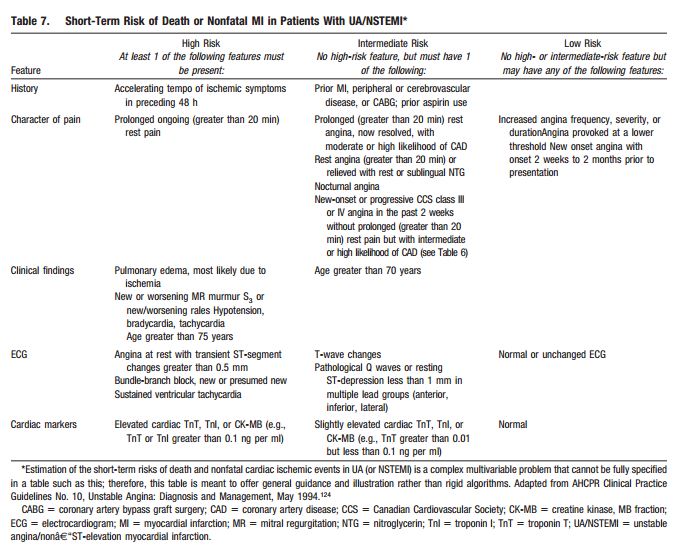
The next important step is to estimate the patient’s risk of death or nonfatal MI, the GRACE risk score is one way to do this (discussed in a previous post), another is Table 7 (p e442) in the Guidelines:
Resources:
Global Registry of Acute Coronary Events
GRACE ACS Risk Model: Calculator Instructions GRACE Info Reference



