5.3. Laboratory Measurement (continued)
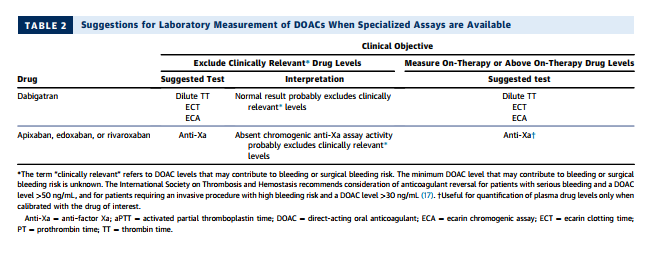
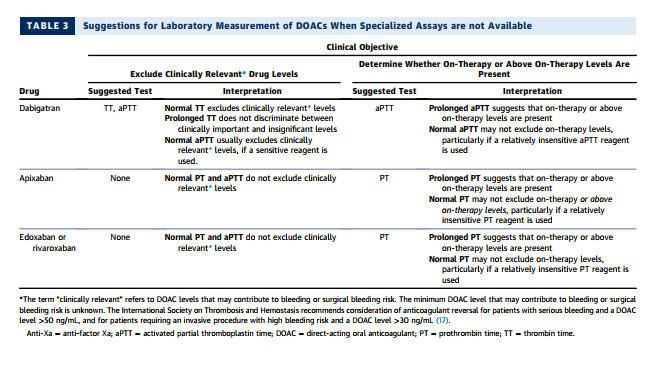
The best tests for assessing the anticoagulant activity of dabigatran include the dilute thrombin time, ecarin clotting time, and ecarin chromogenic assay (see Table 2) (18,19). These tests correlate closely with dabigatran levels measured by the reference standard method, liquid chromatography-tandem mass spectrometry. Unfortunately, these assays are not widely available, particularly on an emergent basis (18,19). In their absence, the thrombin time (TT) and aPTT may be used for qualitative assessment (see Table 3). The TT is exquisitely sensitive to dabigatran, even at very low drug concentrations. Thus, a normal TT excludes clinically relevant dabigatran levels, but a prolonged TT does not discriminate between clinically important and insignificant drug concentrations. All laboratories that do not offer an around-theclock assay for dabigatran quantification should be encouraged to offer the TT for rapid exclusion of clinically significant dabigatran levels. A prolonged aPTT suggests the presence of on-therapy or above on-therapy levels of dabigatran. However, a normal aPTT does not exclude the presence of on-therapy levels, especially when a relatively insensitive aPTT reagent is used (16,18,19)
The preferred test for assessing the anticoagulant activity of apixaban, edoxaban, and rivaroxaban is a chromogenic anti-Xa assay (see Table 2) (18,19). When the assay is calibrated with the drug of interest, the results correlate closely with plasma drug levels measured by liquid chromatography-tandem mass spectrometry. When the assay is calibrated with a low-molecular-weight heparin standard, it can be useful for excluding clinically important levels of drug, but not for quantitation. If an anti-Xa assay is not available, the PT may be useful for qualitative assessment of edoxaban and rivaroxaban. A prolonged PT suggests on-therapy or above on-therapy levels for these agents. However, depending on the sensitivity of the PT reagent, a normal PT may not exclude on-therapy levels (18,19). The PT and aPTT are insensitive to apixaban. A prolonged PT suggests the presence of clinically important apixaban levels, but a normal PT and aPTT do not exclude on-therapy or even above on-therapy levels of the drug (18–20).