
In addition to the Curbsiders’ post below, please review:
- Tuberculosis Screening, Testing, and Treatment of U.S. Health Care Personnel: Recommendations from the National Tuberculosis Controllers Association and CDC, 2019 [Full Text HTML] [Full Text PDF] . Morbidity and Mortality Weekly Report (MMWR). Weekly / May 17, 2019 / 68(19);439–443.
- Official American Thoracic Society/Infectious Diseases Society of America/Centers for Disease Control and Prevention Clinical Practice Guidelines: Diagnosis of Tuberculosis in Adults and Children [Full Text HTML] [Full Text PDF]. Clinical Infectious Diseases® 2017;64(2):e1–e33
- Tuberculosis, Page last reviewed: December 31, 2018, Centers for Disease Control and Prevention
In this post I link to and excerpt from The Curbsiders’ #178 Tuberculosis Updates with Laila Woc-Colburn MD. OCTOBER 21, 2019. OCTOBER 21, 2019. By Hannah Abrams.
Here are excerpts:
Time Stamps
- 00:00 Sponsor: ACP’s National Internal Medicine Day I.M. Proud Story Contest
- 00:24 Disclaimer, Intro, Guest bio, Pun
- 03:51 Guest one-liner, Career Advice; Picks of the Week*: Leonardo Da Vinci by Walter Isaacson; Aditya Shah (@IDdocAdi) antibiotic stewardship on Twitter; @EpicEMRParody on Twitter; Zima is a presumably delicious beverage (we’ve never tried it…ha)
- 09:52 Sponsor: ACP’s National Internal Medicine Day I.M. Proud Story Contest
- 11:30 Case of latent TB; Interpretation of PPD (Tuberculin Skin Test)
- 17:05 PPD and BCG vaccine; Who needs an IGRA?
- 19:20 LTBI treatment threshold; IGRA explained including what to do with “indeterminate results”
- 25:22 LTBI natural history; Why endemic countries don’t treat LTBI
- 30:08 TB infection, immunity and reinfection
- 33:33 How to counsel patients about latent tuberculosis treatment
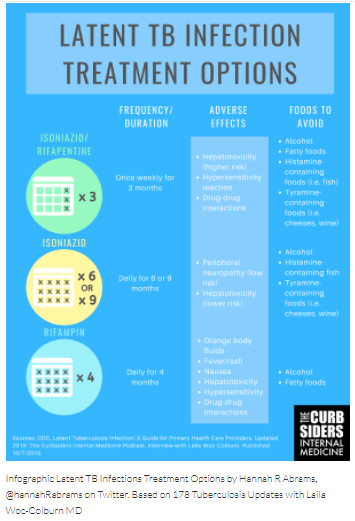
- 38:25 Dietary and alcohol restrictions during LTBI therapy
- 44:18 Screening of healthcare workers
- 48:02 Case of active TB; AFB smears and nucleic acid amplification tests
- 56:05 Initiation of antibiotics for tuberculosis and how to handle TB resistance
- 58:13 Airborne precautions; Who needs them and how to isolate patients
- 61:24 Direct observed therapy and why adherence to tuberculosis therapy is challenging
- 68:11 Tuberculosis UV light and sanatoriums
- 71:00 Take home points
- 72:25 Outro
Tuberculosis Pearls
- 2019 CDC guidelines no longer recommend annual PPD or IGRA for all health care workers. Instead, there is an increased emphasis on occupational exposure education.
- Isoniazid/Rifapentine is a new once-weekly treatment option for latent TB infection that can reduce overall treatment time to 12 weeks. Key adverse effects are hepatotoxicity and drug-drug interactions.
- Consider HIV testing in all patients suspected of having active TB disease.
- If you are unsure if your patient may have TB disease, Dr. Woc-Colburn recommends: err on the side of caution and isolate.
Tuberculosis Show Notes
Latent Tuberculosis
Latent tuberculosis infection (LTBI) occurs when macrophages wall off the mycobacterium and prevent it from spreading. Dr. Woc-Colburn recommends thinking of host defenses here as a real wall: if something occurs to prevent the body from doing regular maintenance on the wall (immunosuppression or age-related immunosenescence), LTBI can become active TB.
Screening for Health Care Workers
Goodbye to the annual PPD? The 2019 CDC guidelines for health care personnel screening [Full Text HTML] [Full Text PDF] include big changes to annual screening and strengthen recommendations for TB occupational hazard education.
BASELINE SCREENING
Previous guidelines recommended all new health care personnel be screened with a PPD (Tuberculin Skin Test) or IGRA (Interferon Gamma Release Assay). The new guidelines recommend a baseline risk assessment asking about TB exposure, travel to endemic regions, and history of immunosuppression to inform test interpretation. Greater emphasis is also placed on annual education for all providers on occupational exposures to TB. (Sosa 2019)
ANNUAL SCREENING
Serial screening is no longer routinely recommended for health care providers without LTBI, but can be considered for groups at high risk such as pulmonologists and respiratory therapists who may have ongoing exposure. (Sosa 2019)
POST-EXPOSURE TESTING
Symptom evaluation is recommended for all health care providers with a suspected exposure. For providers with no history of LTBI or TB disease, testing should be done immediately and, if negative, repeated after 8-10 weeks. (Sosa 2019)
Diagnostics
Dr. Woc-Colburn walks us through interpretation of the PPD (purified protein derivative) or TST (Tuberculin Skin Test) and IGRA (Interferon-Gamma Release Assay.)*
*I ordered a transcript and will paste this in here.
INTERPRETING THE PPD: INDURATION
PPDs should be read 48-72 hours after placement (don’t place them on Thursday!) by induration. Guidelines for diagnosing LTBI based on PPD induration remain unchanged, with the following cutoffs for various patient groups:
5mm: Patients with HIV, immunosuppression, nodular or fibrotic changes on chest X-ray, or recent contact with known active TB infection. (CDC 2016) Immunosuppression includes organ or stem cell transplant recipients, stem cell transplant recipients, patients on TNF-alpha antagonists, or on long-term prednisone > 15 mg/day. (CDC 2016)



