
Emergency Medicine Cases has two great teaching podcasts on Atrial Fibrillation: Case 20 Atrial Fibrillation [link is to the show notes and to the podcast] and Episode 57: The Stiell Sessions 2 – Update in Atrial Fibrillation 2014 [link is to the show notes and to the podcast]. Dr Himmel advises that we all first listen to and review Case 20 podcast and show notes which has all the basics of AF up to 2012 and then listen to and review Episode 57.
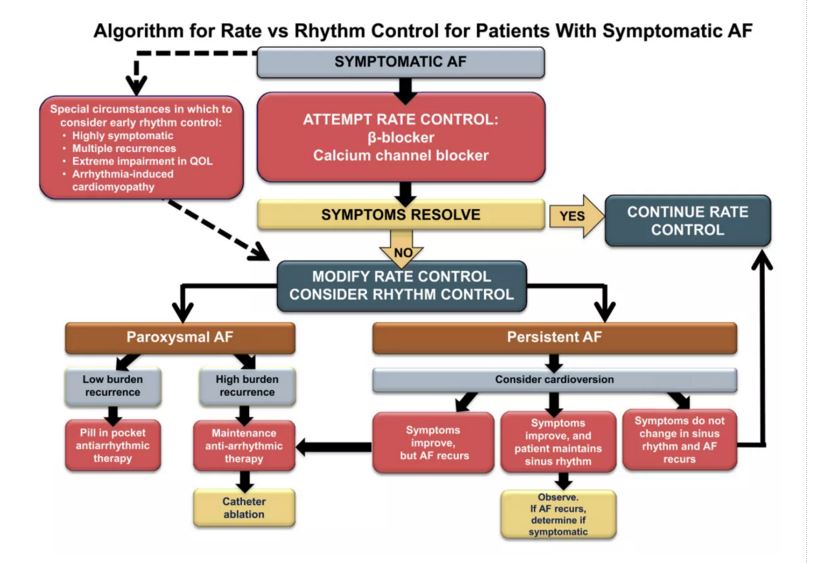
There are two charts on rhythm control vs. rate control from Case 57 show notes included just prior to the Resources.
In Resources, there are links to references and critical updates included in the Case 57 show notes that need to be reviewed.
Case 20 Atrial Fibrillation [link is to the show notes and to the podcast] from Emergency Medicine Cases is the best way to review the diagnosis and management of atrial fibrillation. The podcast and show notes are just outstanding – worth reviewing whenever you see an AF patient unless you see them every day. See also the excellent PDF notes on Case 20.
In the podcast, the doctors state that effective anticoagulation cuts the risk of stroke from atrial by 70% [And 15 to 25% of all strokes are thought to be due to atrial fibrillation].
The following are just a few quotes from the podcast:
[In an unstable patient in A. fib] A.fib is rarely the sole cause of a patient’s hemodynamic instability, so look for another cause – sepsis, hemorrhagic (GI, AAA), dehydration, etc [so cardioversion very well may not work – rather try to treat the secondary cause of the instability and try to avoid cardioversion, if you can].
Etiology or Precipitants of Atrial Fibrillation
PIRATES – PE, Ischemia, Respiratory disease, Atrial enlargement or myxoma, Thyroid disease (check TSH and free T4 in first-time presenters), Ethanol (“Holiday heart” after binging), Sepsis or Sleep apnea
Others include myocarditis and chronic hypertension
Etiology of Slow A.fib: AV nodal blocking agents (digoxin, beta-blocker or calcium-channel blocker toxicity or at too high doses), sick sinus syndrome and severe hyperkalemia [the speakers remind us to always think of hyperkalemia as a cause of bradycardia and get a serum potassium stat (i-stat if you have one)].
1/3 are ‘lone Afib’ with no demonstrable cause
In most cases, when the underlying cause is addressed the A.fib resolves
Two Charts from Case 57 show notes: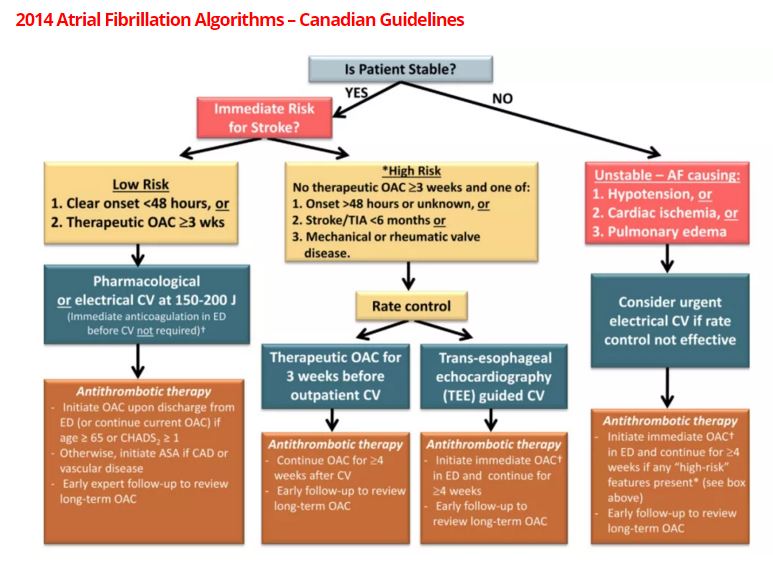
Resources [all are from show notes of Case 57]
Case 57: Published December 2014
Link to Episode 20 on Atrial Fibrillation with Dr. Clare Atzema, Nazanin Meshkat & Bryan Au on the pearls, pitfalls, ins and outs of Atrial Fibrillation to 2012.Dr. Stiell’s blog post on the Canadian Cardiovascular Society CHADS-65 Risk Stratification Algorithm
Dr. Stiell’s blog post on ED Treatment Algorithm for Anticoagulants in Atrial Fibrillation
Dr. Stiell’s blog post on Unstable Patients with Atrial Fibrillation
Canadian Atrial Fibrillation Guidelines 2014 Full PDF
American Heart Association Atrial Fibrillation Guidelines 2014 Full PDF
AFFIRM trial on rate control vs rhythm control
JACC Finnish study on Thromboembolic Complication After Cardioversion of Acute Atrial Fibrillation that challenges the 48 hour safety rule
The Ottawa Aggressive Protocol for cardioversion of Atrial Fibrillation with Procainamide
Update 2015: A viewpoint article in the Canadian Journal of Cardiology by Stiell et al. on the safety of urgent cardioversion in recent onset atrial fibrillation and flutter, in light of the Finnish study. Abstract
![]() Update 2015: A 30-day mortality clinical decision instrument for patients who present to the ED with AFib.Abstract
Update 2015: A 30-day mortality clinical decision instrument for patients who present to the ED with AFib.Abstract
For Clare Atzema’s Best Case Ever on Atrial Fibrillation go to Best Case Ever 7



