
Recently a friend, not a patient, was found to have mildly elevated liver enzymes ( AlT 92 [7-52], AST 74 [N 13-39]) and a mildly decreased estimated Creatinine Clearance of 49 (N is greater than or equal to 60).
Her doctor repeated the labs, ordered a liver ultrasound scan and referred her to a gastroenterologist – the tests and consult are pending.
Her question was what could these abnormal labs mean? And could the abnormal liver and kidney test be serious?
Today I’m going to review the evaluation of an abnormal estimated creatinine clear using Chronic Kidney Disease: Detection And Evaluation from the American Family Physician [Resource (1) below].
After I finish the article review, I will list my thoughts on what further evaluation is indicated for my friend’s abnormal estimated created clearance.
Tomorrow I’ll review the evaluation of abnormal liver function tests.
So what follows are excerpts from Resources (1), Chronic Kidney Disease: Detection And Evaluation:
Abstract:
Chronic kidney disease affects 47 million people in the United States and is associated with significant health care
costs, morbidity, and mortality. Because this disease can silently progress to advanced stages, early detection is critical for initiating timely interventions. Multiple guidelines recommend at least annual screening with serum creatinine, urine albumin/creatinine ratio, and urinalysis for patients with risk factors, particularly diabetes mellitus, hypertension, and a history of cardiovascular disease. The U.S. Preventive Services Task Force found insufficient evidence to assess the balance of benefits and harms of screening for chronic kidney disease in the general population, and the American College of Physicians recommends against screening asymptomatic adults without
risk factors. Persistently elevated serum creatinine and albuminuria are diagnostic and prognostic hallmarks of
chronic kidney disease. Lower levels of albuminuria are associated with adverse renal and cardiovascular outcomes.
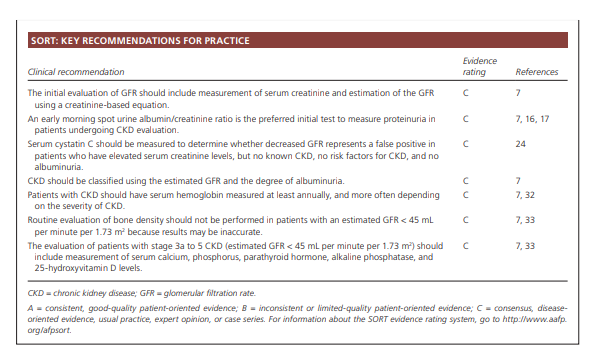
Serum cystatin C is a novel biomarker that is most useful when a false-positive decreased estimated glomerular filtration rate calculated from serum creatinine is suspected [When estimated GFR calculation reveals a value between 45 and 59]. New guidelines incorporate albuminuria into the classification framework for chronic kidney disease and elaborate on identification of the disease, the frequency of follow-up, and recommendations for nephrology referral. Nephrology consultation is indicated for patients with an estimated glomerular filtration rate less than 30 mL per minute per 1.73 m2, persistent urine albumin/creatinine ratio greater than 300 mg per g or urine protein/creatinine ratio greater than 500 mg per g, or if there is evidence of a rapid loss of kidney function. A multidisciplinary approach between primary care physicians, nephrologists, and other subspecialists for implementing early interventions, providing education, and planning for advanced renal disease is key for effective management. (Am Fam Physician. 2017;96(12):776-783. Copyright © 2017 American
Academy of Family Physicians.)
Detection of CKD
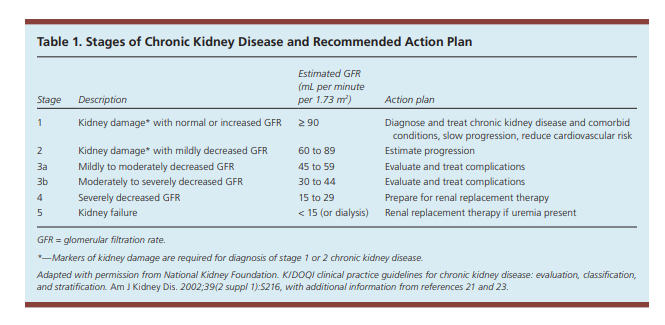
CKD is defined as abnormal kidney structure
or function lasting more than three months with associated health implications.7 Indicators include albuminuria, urine sediment abnormalities, abnormal renal imaging findings, serum electrolyte or acid-base derangements, and glomerular filtration rate (GFR) less than 60 mL per minute per 1.73 m2.7Because CKD can progress to advanced renal failure, end-stage renal disease, and even death, early detection is critical for initiating timely therapeutic interventions, limiting nephrotoxin exposure, preventing further reduction in GFR, and preparing for renal replacement therapy.8,9
Screening Indications:
Multiple guidelines recommend that patients with diabetes
or hypertension be screened annually for CKD. Furthermore, patients with other risk factors, including cardiovascular disease, older age, history of low birth weight, obesity, and a family history of CKD, warrant consideration for screening.7,10,11Screening Tests:
Screening for CKD includes measurement of serum creatinine,
estimation of GFR using a serum creatinine based equation, measurement of the urine albumin/creatinine ratio, and urinalysis.7. . . . Because albumin is the predominantly filtered glomerular protein, initial proteinuria evaluation using the spot urine albumin/creatinine ratio obtained from an early morning sample is recommended.7,16,17GFR Estimation
Steady state renal function is best determined by estimation
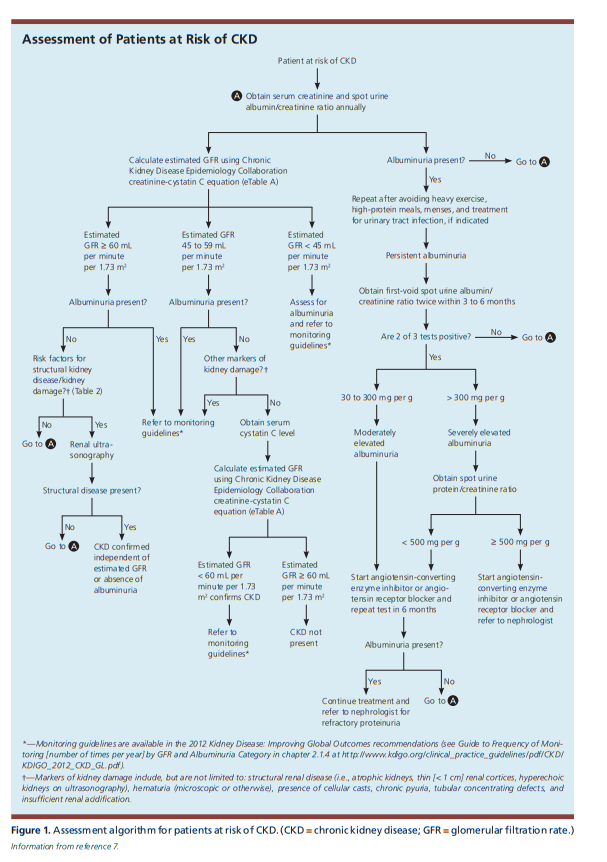
of GFR, which is derived from measurement of serum creatinine.Serum cystatin C is a filtration marker that has emerged as an alternative to serum creatinine to more accurately estimate GFR and classify CKD. Obtaining the serum cystatin C–based estimated GFR is most beneficial when a false-positive decreased estimated GFR is suspected, such as in a patient without known structural kidney disease, risk factors for CKD, or albuminuria who has a creatinine clearance–calculated estimated GFR of 45 to 59 mL per minute per 1.73 m2 24 In
such cases, the serum cystatin C and serum creatinine levels can be obtained concurrently for recalculation of the estimated GFR using the appropriate calculator7,24,25 (eTable A). If the estimated GFR calculated using both serum creatinine and serum cystatin C is greater than 60 mL per minute per 1.73 m2, a diagnosis of CKD is not warranted. A recent community-based longitudinal observational study demonstrated that a reduced serum cystatin C–based estimated GFR was associated with all cause and cardiovascular disease mortality.26 It should be noted that serum cystatin C is not reliable in patients
with acute kidney injury, inflammatory states, or thyroid dysfunction.7,16,25,27 Furthermore, it is not yet universally
available and may add significant cost to the evaluation.
For patients whose initial estimated GFR (using the standard calculation that the lab gives you) is between 45 to 59 ml per minute per 1.73 meters squared, repeat the serum creatinine and at the same time obtain a serum cystastin C level. Plug these values into the GFR Calculator from the National Kidney Foundation.
Once reduced GFR and/or presence of proteinuria are
determined to be chronic and stable (unchanged for more
than three months), a comprehensive initial workup is
necessary to determine the etiology of CKD. Etiologies
include hypertensive kidney disease, diabetic nephropathy,
or primary or secondary glomerulonephritis.7
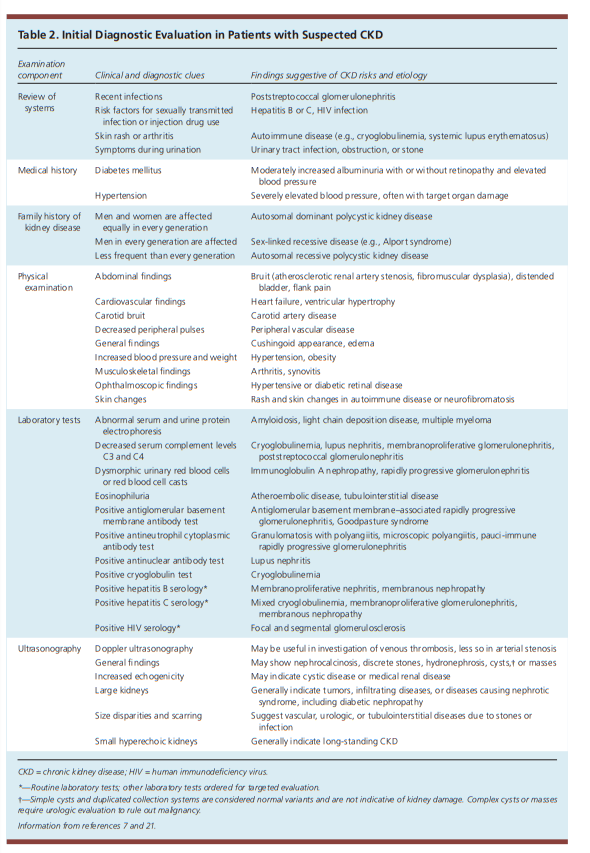
A full medical history, including exposure to potential nephrotoxins; physical examination; and review of historical
and current blood pressure, dietary history, and
weight measurements are essential for CKD evaluation7
(Table 2 7,21).
Laboratory assessment should include measurement of serum electrolytes, fasting lipids, A1C, and urine albumin/creatinine ratio.7 Urinalysis with microscopic urine sediment is helpful if intrinsic renal disease is suspected.21 Renal ultrasonography is recommended to evaluate for structural abnormalities.30 Figure 1 outlines a proposed approach to the evaluation of CKD.
See Table 3. Clinical Interventions For Adults With Chronic Kidney Disease, p. 781.
So here is my take on what I as primary care physician would do for a patient who was found to have an estimated creatinine clearance of 49.
I would order a repeat serum creatinine and add a serum cystastin C test. And with these two tests I would be able to calculate a serum cystatin C–based estimated GFR by plugging these values into the GFR Calculator from the National Kidney Foundation. It turns out that the initial simplified GFR calculation used by the lab can be falsely low when the value is between 45 and 59. It is in this situation that we would calculate the serum cystastatin C-based estimated GFR.
As the authors remind us:
It should be noted that serum cystatin C is not reliable in patients with acute kidney injury, inflammatory states, or thyroid dysfunction.7,16,25,27 Furthermore, it is not yet universally available and may add significant cost to the evaluation.*
*For guidance on the diagnosis and management of Acute Kidney Injury see my post Guidelines For The Diagnosis and Management Of Acute Kidney Injury
Posted on August 13, 2018.
I would also order an early morning spot urine for albumin/creatinine ratio, and a urinalysis with microscopy.
If any of the above three tests are abnormal, I would refer to nephrology for further evaluation. It would not be unreasonable to instead refer a standard estimated creatinine based GFR of 45 to 59 to a nephrologist for the above tests.
Resources:
(1) Chronic Kidney Disease: Detection And Evaluation [PubMed Abstract] [Full Text HTML] [Full Text PDF] Article currently embargoed except for subscribers. The full text links will only work on my account as I purchased the article for $14.95 (worth it).
(2) KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease [Full Text PDF]. From volume 3 | issue 1 | JANUARY 2013
https://www.kidney-international.org.



