
In this post, I link to and excerpt from Autonomic dysfunction in ‘long COVID’: rationale, physiology and management strategies [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Clin Med (Lond). 2021 Jan; 21(1): e63–e67.
The above article has been cited by 111 articles.
All that follows is from the above article.
ABSTRACT
The SARS-CoV-2 (COVID-19) pandemic has caused unprecedented morbidity, mortality and global disruption. Following the initial surge of infections, focus shifted to managing the longer-term sequelae of illness in survivors. ‘Post-acute COVID’ (known colloquially as ‘long COVID’) is emerging as a prevalent syndrome. It encompasses a plethora of debilitating symptoms (including breathlessness, chest pain, palpitations and orthostatic intolerance) which can last for weeks or more following mild illness. We describe a series of individuals with symptoms of ‘long COVID’, and we posit that this condition may be related to a virus- or immune-mediated disruption of the autonomic nervous system resulting in orthostatic intolerance syndromes. We suggest that all physicians should be equipped to recognise such cases, appreciate the symptom burden and provide supportive management. We present our rationale for an underlying impaired autonomic physiology post-COVID-19 and suggest means of management.
KEYWORDS: orthostatic, dizziness, dysautonomia, COVID-19, long COVID‘Long COVID’ and orthostatic intolerance syndromes
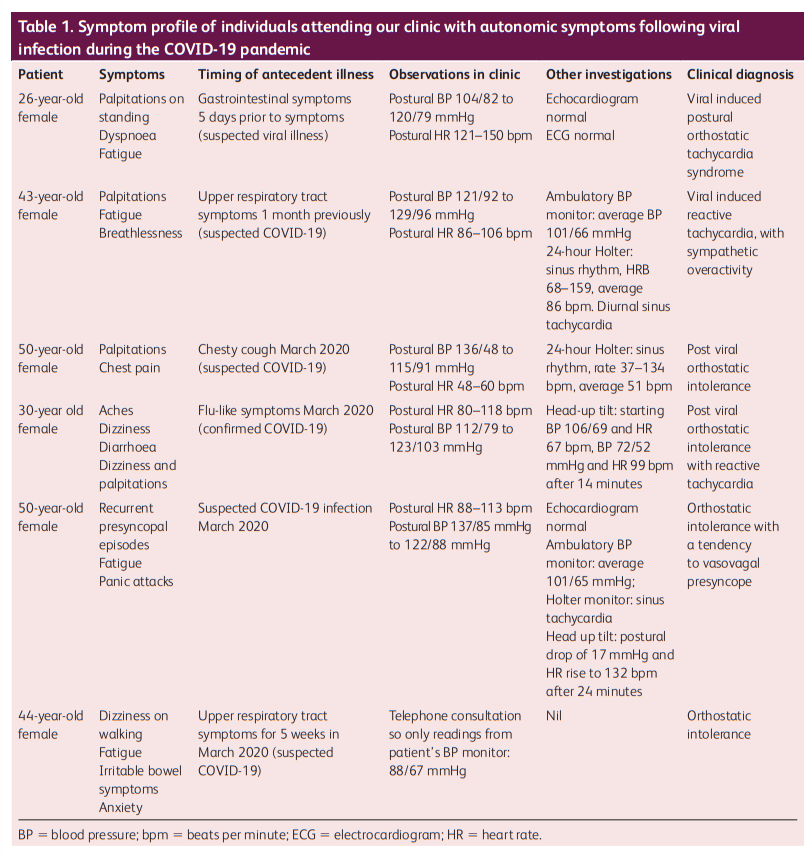
In our tertiary syncope unit, we have encountered patients with debilitating symptoms following viral infections who were subsequently found to have orthostatic intolerance syndromes. A summary is shown in Table Table1.1. While only one case in this series had confirmed COVID-19, the others had symptoms consistent with a debilitating viral illness in early 2020 and were suspected cases during a period where COVID testing was not recommended or widely available. Of note, all of the individuals in this short series were female and were between the ages of 26 and 50 years old. They all had orthostatic intolerance with either resting or postural hypotension and/or tachycardia. We propose that some symptoms of the so-called ‘long COVID’ infection may be related to a virus- or immune-mediated disruption to the autonomic nervous system, resulting in transient or long-term orthostatic intolerance syndromes.
Introduction
Results of the COVID Symptom Study (based on a smartphone
tracker app where users enter their symptoms, which had over
2.8 million recorded users by May 2020)3,4 are awaited, but smaller studies reveal that protracted symptoms following COVID-19 infection are common. In Italian inpatients, 53% had fatigue, 43% were dyspnoeic and 22% were experiencing chest pain after 2 months.2 Halpin et al reported that after 4–8 weeks, ongoing fatigue is present in more than two thirds, followed by breathlessness and symptoms of post-traumatic stress disorder.5 Mainstream media are giving publicity to patient-coined terms ‘long COVID’6
and ‘long-haul COVID’.7 The popularity and visibility
of patient support groups such as wearebodypolitic.com (who
according to their website have 14,000 subscribers) and the Long COVID SOS group (longcovidsos.org), and the frequent trending of the hashtag #longcovid on Twitter, suggest that patient need is high, and under-recognised by clinicians.‘Long COVID’ and orthostatic intolerance syndromes
In our tertiary syncope unit, we have encountered patients
with debilitating symptoms following viral infections who were
subsequently found to have orthostatic intolerance syndromes. A summary is shown in Table 1.
While only one case in this series had confirmed COVID-19, the others had symptoms consistent with a debilitating viral illness in early 2020 and were suspected cases during a period where COVID testing was not recommended or widely available. Of note, all of the individuals in this short series were female and were between the ages of 26 and 50 years old. They all had orthostatic intolerance with either resting or postural hypotension and/or tachycardia. We propose that some symptoms of the so-called ‘long COVID’ infection may be related to a virus- or immune-mediated disruption to the autonomic nervous system, resulting in transient or long-term orthostatic intolerance syndromes.
Orthostatic intolerance syndromes include orthostatic
hypotension (OH), vasovagal syncope (VVS) and postural
orthostatic tachycardia syndrome (POTS). The pathophysiology
hinges on an abnormal autonomic response to orthostasis
(standing up). When a healthy person stands, blood pools in
the pelvis and legs, reducing venous return to the heart. This is
detected by baroreceptors in the heart and aorta, which respond
by increasing sympathetic neural and adrenergic tone (mediated by norepinephrine and epinephrine respectively). This results in tachycardia (thus compensating for reduced stroke volume). This is then followed by vasoconstriction in the splanchnic vascular bed, which increases venous return to the heart.In orthostatic intolerance, the release of epinephrine and
norepinephrine causes pronounced tachycardia, which is
experienced as palpitations, breathlessness and chest pain
(common symptoms of ‘long COVID’). Very high catecholamine
levels can lead to paradoxical vasodilatation, sympathetic
activity withdrawal and activation of the vagus nerve resulting in hypotension, dizziness and ultimately syncope.8–11These syndromes may be exacerbated by hypovolaemia resulting from the initial infection or due to deconditioning by bedrest. Prolonged bedrest (there have been extensive studies of head-downbedrest simulating chronic weightlessness in astronauts) leads to reduced cardiac output and stroke volume, hypovolaemia, baroreflex impairment, and withdrawal of the sympathetic neural response.12–15
COVID-19, autoimmunity and the autonomic
nervous systemIt has been hypothesised that COVID-19 infection affects the
autonomic nervous system.16 The relationship between the two
is complex: the well-documented cytokine response storm of
COVID-1917 results from sympathetic activation inducing proinflammatory cytokine release.18,19 Conversely, vagal stimulation results in an anti-inflammatory responses,17 suggesting possible therapeutic targets in the autonomic nervous system.Alternatively, COVID-19 related autonomic dysfunction could
be mediated by the virus itself. Immune-mediated neurological
syndromes have been described.20 It is also well established that autonomic disorders such as OH and POTS are associated
with autoantibodies,21 for example to α-/β-adrenoceptors and
muscarinic receptors.22–25 Cohort studies describe commonly
preceding infections in POTS,26 as well as a link with autoimmune biomarkers and autoimmune disorders.27 Thus, we speculate that there is an underlying autoimmune component to the post-COVID syndromes that we report.
Identifying autonomic dysfunction following COVID-19 infection
Any individuals presenting with breathlessness, palpitations,
fatigue, chest pain, presyncope or syncope should be evaluated
carefully. Cardiovascular, respiratory and neurological
examination with vital signs and pulse oximetry are essential.
Electrocardiogram, blood tests and imaging should be consideredvto identify other important diagnoses such as organisingpneumonia, pulmonary embolism and myocarditis.
An active stand test should be undertaken, measuring blood
pressure and heart rate after 5 minutes lying supine, and then
3 minutes after standing. Orthostatic hypotension is defined as a fall of >20 mmHg systolic and >10 mmHg diastolic after standing for 3 minutes.28 POTS is characterised by orthostatic symptoms (in the absence of orthostatic hypotension) with an increase in heart rate of 30 beats per minute or more when standing for more than 30 seconds, or 40 beats per minute or more in those aged 12–19 years.29
A continuous blood pressure and heart rate trace during a tilt
table test of an individual with orthostatic intolerance post-COVID is shown in Fig 1.
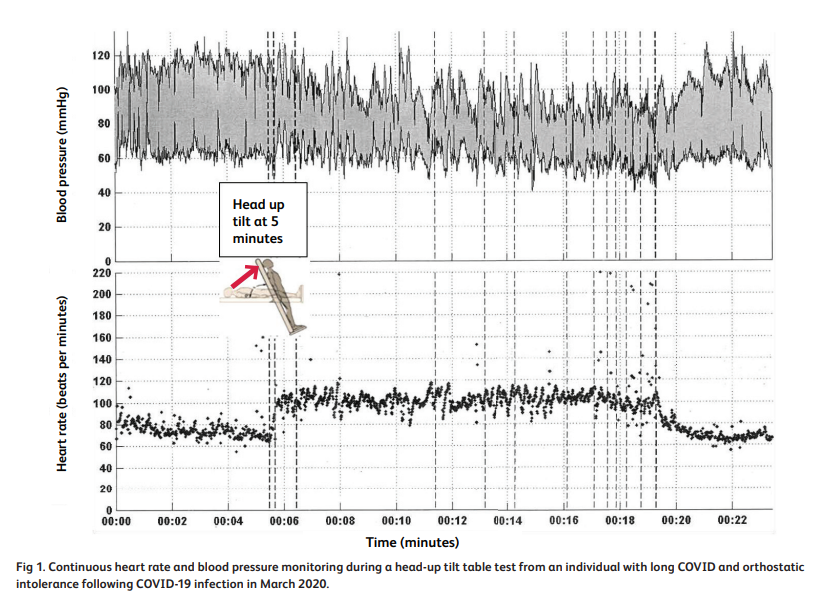
After adopting the upright position, a marked and continuous rise in heart rate was seen, corresponding with the onset of clinical symptoms and mirrored by blood pressure oscillations in keeping with an adrenergic response. The average heart rate rise was under 30 beats per minute, thus not fulfilling criteria for POTS.
Management of orthostatic intolerance
We suggest the following methods of management. This is based
on published international guidance, consensus statements, and
the authors’ own experience and practice in managing orthostatic intolerance syndromes.8,29–31
hypotension: JACC State-of-the-Art Review. J Am Coll Cardiol
2018;72:1294–309.
Society expert consensus statement on the diagnosis and
treatment of postural tachycardia syndrome, inappropriate sinus
tachycardia, and vasovagal syncope. Heart Rhythm 2015;
12:e41–63.
30 Shen WK, Sheldon RS, Benditt DG et al. 2017 ACC/AHA/HRS
guideline for the evaluation and management of patients with
syncope: executive summary. Circulation 2017;136:e25–e59.
31 Brignole M, Moya A, de Lange FJ et al. 2018 ESC Guidelines
for the diagnosis and management of syncope. Eur Heart J
2018;39:1883–48.
Education
Education, explanation and reassurance provide the cornerstone of management of orthostatic intolerance syndromes. Managing the uncertainty associated with COVID-19 and explaining the underlying physiological changes can reassure the patient that their symptoms are not sinister. Reproducing symptoms, for example while on a tilt table, can be effective for explaining symptom correlations with heart rate and blood pressure variations. The patient should be directed to further education sources, such as those from the STARS initiative (Syncope Trust and Reflex Anoxic Seizures) from the Heart Rhythm Alliance (www.heartrhythmalliance.org/stars/uk/), and the authors’ free educational website, www.stopfainting.com.
ExerciseAfter medical examination, we suggest a regular, structured
exercise programme with both aerobic and resistance elements.
As orthostasis (the upright position) may be problematic, nonupright exercise such as cycling on a recumbent exercise bike and swimming are encouraged.
Fluid and salt repletionEnsuring fluid repletion (2–3 litres water per day and avoiding
caffeine and alcohol) and ensuring one to two teaspoons of salt
supplementation per day helps maintain plasma volume and
avoid hypovolaemia.
Avoiding exacerbating factorsThe patient should be advised on rising cautiously from a lying
or seated position and avoiding exacerbating factors such as
prolonged standing, warm environments and dehydration.
Additionally, patients can be advised to consume small and frequent rather than large meals to avoid splanchnic vasodilatation.
Isometric exercisesSimple physical isometric counter-manoeuvres can be taught
to those with orthostatic hypotension. These simple exercises
involve sustained tensing of muscles which increases venous return to the heart and raises blood pressure. These counter-pressure manoeuvres include tensing thigh and buttock muscles, crossing arms and legs, folding arms and leaning forward, squatting, or raising a leg and placing the foot on a stool.
Compression garmentsIn orthostatic hypotension, compression garments extending up
to the waist, or abdominal binders, are effective and tolerable.
Pharmacological treatmentIf POTS features are present, norepinephrine reuptake inhibitors such as duloxetine, nortryptiline and tapentadol should be discontinued if possible.29
If symptoms persist despite full compliance with conservative
measures, pharmacological therapy may be considered.Fludrocortisone, a fluid expander, can be used if hypovolaemia is considered to be a dominant symptom. It is associated with side effects and not particularly well tolerated. Monitoring should take place for fluid retention and hypokalaemia.
Midodrine, a sympathomimetic α-1-agonist, increases
vasoconstriction and venous return to the heart. It can effectively treat orthostatic hypotension and tachycardia in patients who have a baseline normal or low-normal blood pressure. Patients should be advised to avoid the supine position as much as possible, thereby reducing the tendency to excessive blood pressure rise in this position. Urinary retention may be seen in male symptoms with prostatic symptoms and scalp itch are common side effects.
For prominent hyperadrenergic symptoms caused by the
catecholamine surge on standing, clonidine and methyldopa
may alleviate symptoms. Similarly, propranolol can attenuate
palpitations and tachycardia.8,29–31 However, none of these agents is well tolerated.
ConclusionSeveral months on from the declaration of the COVID-19 pandemic, new symptom patterns and syndromes such as ‘long COVID’ are emerging. These patterns may be explained by autonomic instability and may result from deconditioning, hypovolaemia or immune- or virus-mediated neuropathy. We anticipate that these syndromes will represent a large proportion of primary and secondary care consultations in coming months. Clinicians must be aware that prompt and correct diagnosis with careful management are essential for recovery. ■



