In this post, I link to and excerpt from Diagnosis and treatment of primary aldosteronism: practical clinical perspectives [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. J Intern Med. 2019 Feb;285(2):126-148.
All that follows is from the above article.
Abstract
Primary aldosteronism (PA), the most common form of secondary hypertension, can be either surgically cured or treated with targeted pharmacotherapy. PA is frequently undiagnosed and untreated, leading to aldosterone-specific cardiovascular morbidity and nephrotoxicity. Thus, clinicians should perform case detection testing for PA at least once in all patients with hypertension. Confirmatory testing is indicated in most patients with positive case detection testing results. The next step is to determine whether patients with confirmed PA have a disease that can be cured with surgery or whether it should be treated medically; this step is guided by computed tomography scan of the adrenal glands and adrenal venous sampling. With appropriate surgical expertise, laparoscopic unilateral adrenalectomy is safe, efficient and curative in patients with unilateral adrenal disease. In patients who have bilateral aldosterone hypersecretion, the optimal management is a low-sodium diet and lifelong treatment with a mineralocorticoid receptor antagonist administered at a dosage to maintain a high–normal serum potassium concentration without the aid of oral potassium supplements.
Introduction
Hypertension, increased adrenal aldosterone secretion and suppressed renin are the three hallmarks of primary aldosteronism (PA), which was first fully described in 1955 1. Although estimates vary 2, the prevalence of PA is approximately 5% in patients with hypertension 3 and up to 20% in those with treatment-resistant hypertension 4, 5. Cardiovascular and cerebrovascular morbidity and mortality rates in patients with PA are increased compared with subjects with apparent essential hypertension matched for age, sex and blood pressure 6–10. The early diagnosis of PA provides the opportunity to either cure hypertension or to direct targeted pharmacotherapy, both of which can prevent end-stage PA (i.e. end-stage renal disease and irreversible cardiovascular damage).
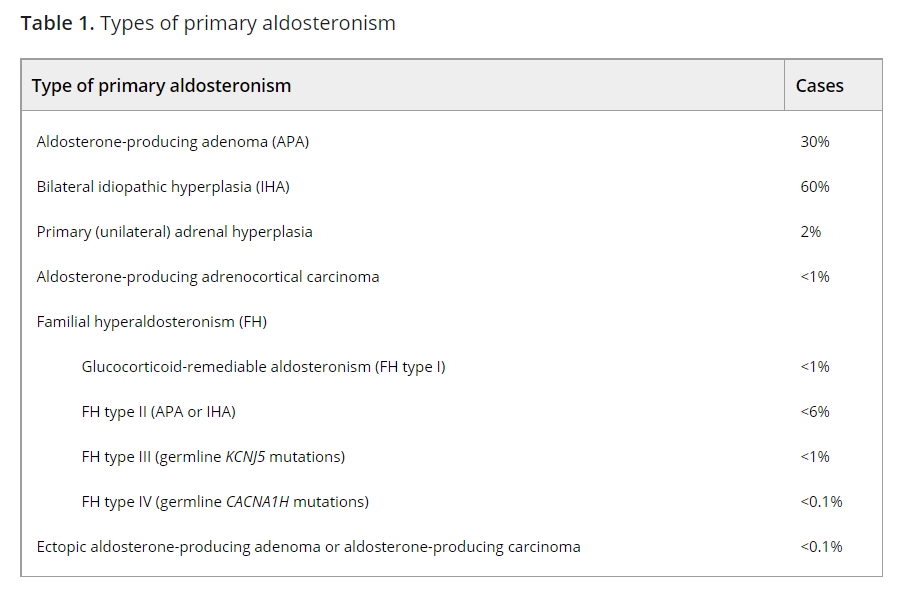
Aldosterone-producing adenoma (APA) and bilateral idiopathic hyperaldosteronism (IHA) are the two most common subtypes of PA (Table 1) 11. A less common form of PA, unilateral hyperplasia or primary adrenal hyperplasia (PAH), is caused by micronodular or macronodular hyperplasia of the zona glomerulosa of predominantly one adrenal gland. Familial hyperaldosteronism (FH) is rare, and germline mutations in four different genes have been described (see section on FH below).
Clinical presentation
Primary aldosteronism is usually diagnosed between 20 and 60 years of age. There is no reliable clinical phenotype to guide the clinician on which patients should be tested for PA. A hypokalaemia-induced renal-concentrating defect can result in polyuria and nocturia; this presentation is frequently mistaken for prostatism in men. The degree of hypertension is typically moderate to severe and may be resistant to usual pharmacologic treatments 12, 13. The mean blood pressure (±SD) was 184/112 ± 28/16 mmHg in the first 262 patients with PA who were diagnosed at Mayo Clinic (1957–1986) 13. In general, patients with APA tend to have higher aldosterone levels and higher blood pressures than patients with IHA. Because hypokalaemia is present in only 28% of patients with PA 14, 15, all patients with hypertension are potential candidates for this disorder. There is a unique subset of young patients (typically <35 years of age) who present with marked hypokalaemia but are not technically hypertensive with systolic/diastolic blood pressures of 130s/80s mmHg. These patients usually have APA and their pre-PA baseline blood pressures average 100/60 mmHg. Thus, although they do not meet the criteria for hypertension, there is a clinically significant change from baseline and presumably their young age and blood pressure counter regulatory mechanisms prevent hypertension, at least in the first year or two of the disease.
The prevalence of target-organ damage to the heart and kidney is increased in patients with PA compared to those with essential hypertension 7, 10, 16. Long-standing undiagnosed PA frequently leads to chronic kidney disease 17. In a recent meta-analysis of 31 studies, including 3838 patients with PA and 9284 patients with essential hypertension, patients with APA and IHA had an increased risk of stroke [odds ratio (OR) 2.58], coronary artery disease (OR 1.77), atrial fibrillation (OR 3.52) and heart failure (OR 2.05) 10. In addition, the diagnosis of PA increased the risk of diabetes (OR 1.33), metabolic syndrome (OR 1.53) and left ventricular hypertrophy (OR 2.29) 10. Thus, the cardiovascular toxicity in PA extends beyond hypertension; there is an aldosterone-specific toxicity.
The risk of developing new-onset diabetes mellitus was also demonstrated in a study of 2367 patients with PA who had no prior diagnosis of diabetes mellitus, in which 754 surgically treated patients with APA were matched with 3016 control subjects with essential hypertension 18. The patients with PA who underwent adrenalectomy had a statistically significant reduced risk for incident diabetes and all-cause mortality compared with matched hypertensive controls 18.
Deep-seated renal cysts are found in up to 60% of patients with PA who have chronic hypokalaemia 19. Because of a reset osmostat, the serum sodium concentration tends to be high–normal or slightly above the upper limit of normal 20. This clinical sign is very useful in the initial assessment for potential PA, especially in patients treated with thiazide diuretics (where the serum sodium concentration tends to be low–normal).
Prevalence
Before 1981, PA was thought to be a rare cause of hypertension 27–33. Over time, it has been shown that most patients with PA are not hypokalaemic 11, 12, 14, 34 and that case detection testing can be completed without stopping antihypertensive medications 35. Case detection testing is performed with a morning venipuncture for the measurement of plasma aldosterone concentration (PAC) and plasma renin activity (PRA) or plasma renin concentration (PRC) 11, 35. Thus, current prevalence estimates for PA are 5–10% of all patients with hypertension 2, 3, 14, 15, 34, 36–39. In a recent study of 1672 unselected patients with hypertension, the prevalence of PA was 5.9% and was associated with the severity of hypertension: 3.9% and 11.8% in patients with stage 1 and stage 3 hypertension, respectively 15.
Who should be screened for PA?
Unlike other adrenal disorders (e.g. Cushing syndrome), there is no typical PA phenotype to guide the clinician to suspect PA. Serum potassium status is not a reliable guide for screening for PA because 72% of patients with PA are normokalemic 11, 14, 15.
In efforts to conserve medical costs and limit the consequences of false-positive case detection testing, the Endocrine Society guidelines on PA 11 recommend testing high-risk groups for PA. These groups include: (i) patients with sustained blood pressure above 150/100 mmHg on each of three measurements obtained on different days; (ii) patients with hypertension resistant to three conventional antihypertensive drugs (including a diuretic) or controlled blood pressure on four or more antihypertensive drugs; (iii) patients with hypertension and spontaneous or diuretic-induced hypokalaemia; (iv) patients with hypertension and adrenal incidentaloma; (v) patients with hypertension and sleep apnoea; (vi) patients with hypertension and a family history of early onset hypertension or cerebrovascular accident at a young age (<40 years); and (vii) all hypertensive first-degree relatives of patients with PA 11. Unfortunately, these guidelines are not followed by practising clinicians. For example, in a recent survey of 500 general practitioners in Italy and Germany, case detection testing for PA was performed in only 7–8% of 3135 patients with hypertension 40. Another study in Italy found that PA was dramatically underdiagnosed and undertreated 41.
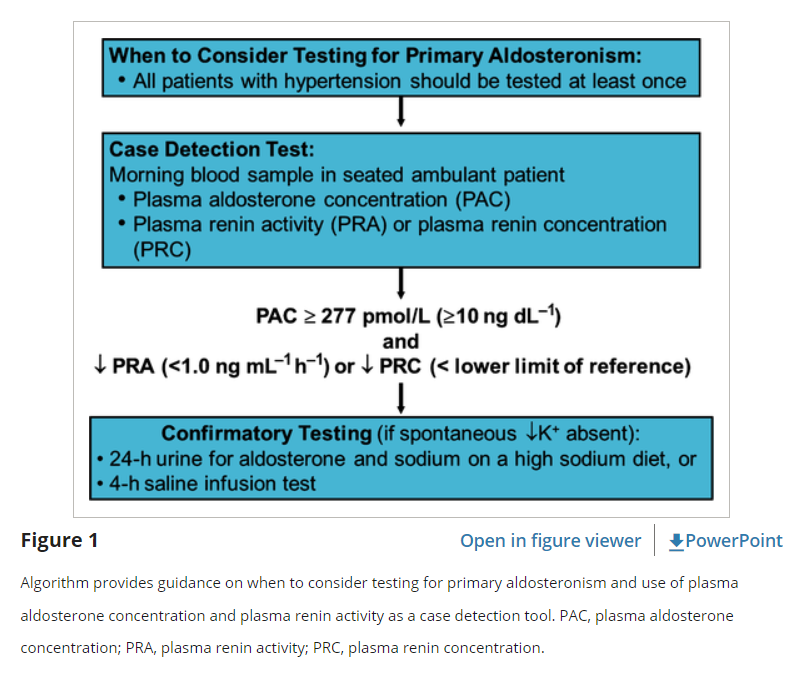
Over more than three decades, it has been frustrating to see patients who were not tested for PA when they were first diagnosed with hypertension, but rather only after they have developed irreversible stage 4 to 5 chronic kidney disease. Clinical practice guidelines have not been effective in driving more clinicians to consider case detection testing for PA 42. Could the guidelines be too complicated with regard to rules on medications and by focusing on recommending subsets of patients for PA testing? The diagnostic algorithm should be simplified, and all patients with hypertension should be recommended for case detection testing for PA at least once (Fig. 1). An initially normal case detection testing result for PA should be repeated if and when there is deterioration in hypertension control 43.
Diagnosis
The diagnosis of PA starts with case detection, followed by confirmatory tests and finally subtype evaluation. Each step may be completed, whilst the patient is taking antihypertensive medications 12. Although hypokalaemia reduces the secretion of aldosterone, it rarely normalizes aldosterone secretion in patients with PA; these patients are hypokalaemic because of excess aldosterone secretion. Nevertheless, restoring the serum potassium level to normal before performing diagnostic studies is optimal (although not necessary in most cases).
The list of drugs and hormones capable of affecting the renin–angiotensin–aldosterone axis in patients without PA is extensive 48. However, it is essential for clinicians to understand that although medications used to treat hypertension can potentially cause false-negative testing results in patients with mild PA, there is no medication that causes false-positive results, as long as a cut-off level for aldosterone is used. Calcium channel blockers and α1-adrenergic receptor blockers do not affect the diagnostic accuracy in most cases 11. Angiotensin-converting enzyme (ACE) inhibitors and angiotensin receptor blockers (ARBs) have the potential to elevate PRA in patients with mild PA. Therefore, the finding of a PRA level ≥1.0 ng mL−1 h−1 or a PRC that is not suppressed in a patient taking an ACE inhibitor or ARB does not exclude the diagnosis of PA. However, a PRA level <1.0 ng mL−1 h−1 or a PRC below the reference range in a patient taking an ACE inhibitor or ARB is diagnostic of low-renin hypertension and possible PA. MRAs (e.g. spironolactone and eplerenone) prevent aldosterone from activating the receptor, resulting sequentially in sodium loss, a decrease in plasma volume and an elevation in renin. If PRA or PRC is not suppressed in a patient treated with an MRA, then no further PA-related testing can be performed and the MRA should be discontinued for 6 weeks before re-testing. However, if the patient is hypokalaemic despite treatment with an MRA, then the mineralocorticoid receptors are not fully blocked and PRA or PRC should be suppressed in such a patient with PA. In addition, in the author’s experience, most patients with PA are treated with suboptimal dosages of MRAs and the mineralocorticoid receptors are not fully blocked. Thus, for case detection testing, blood pressure medications, including MRAs, should not be discontinued. Clinicians can proceed with case detection testing in all patients treated with MRAs, and the MRA does not need to be discontinued for confirmatory or subtype testing with adrenal vein sampling (AVS) if PRA or direct renin concentration is suppressed 49. Other potassium-sparing diuretics, such as amiloride and triamterene, usually do not interfere with testing unless the patient is treated with high doses, which may result in elevated PRA or PRC.
Measurement of renin
Renin can be measured based on its enzymatic activity (PRA) or on its mass (PRC). PRA is determined with an enzyme-kinetic bioassay by measurement of angiotensin I generation with a radioimmunoassay and expressed as the amount of angiotensin I generated per unit of time (e.g. ng mL−1 h−1 or nmol L−1 h−1). PRC is measured by an automated immunometric assay that detects both prorenin and renin and is expressed as mU L−150. Normal morning PRA for seated individuals ranges from approximately 1–4 ng mL−1 h−1 (0.8–3.0 nmol L−1 h−1). The corresponding normal reference range for PRC is 8 to 35 mU L−1. For convenience, automation and speed, many clinical laboratories have switched from PRA to PRC assays. In general, there is a good correlation between PRA and PRC 51, 52. However, PRC can be affected by oestrogen status in women. For example, false-positive results on case detection testing for PA can occur when PRC is measured in women receiving oestrogen-containing preparations 48, 53, 54. In addition, the pre-ovulatory surge in oestrogen in premenopausal women is associated with false-positive case detection testing when using PRC, but not PRA 54. Thus, although both methods to measure renin are suitable for case detection testing for PA, use of PRA is preferred.
Case detection tests
Case detection testing involves the measurement of PAC and PRA (or PRC) in a random morning ambulatory blood sample (Fig. 1). In 1981, Hiramatsu and colleagues proposed the PAC/PRA ratio as a case detection test for PA 35. In a patient with hypertension and hypokalaemia, secondary hyperaldosteronism (e.g. renovascular hypertension) should be considered if both PAC and PRA are increased and the PAC/PRA ratio is <277 (with PAC measured in pmol L−1 and PRA in ng mL−1 h−1; PAC/PRA ratio <10 if PAC is measured in ng dL−1 and PRA in ng mL−1 h−1). If both PAC and PRA (or PRC) are suppressed in a patient with hypertension and hypokalaemia, an alternate source of agonism at the mineralocorticoid receptor should be considered (e.g. hypercortisolism, licorice use). Furthermore, PA should be suspected if the PRA is suppressed to <1.0 ng mL−1 h−1 (or PRC below the lower limit of the reference range) and the PAC is inappropriate for the PRA or PRC [e.g. PAC >277 pmol L−1 (>10 ng dL−1)]. Interpretation of the PAC/PRA ratio has proven to be confusing due to the wide variation in the lower limits of detection for PRA. Thus, it is more practical to use absolute values for PAC and renin (PRA or PRC) (Fig. 1). The measurement of PAC and PRA or PRC is widely accepted as the case detection test of choice for PA 11, 55, 56. A PAC >277 pmol L−1 (>10 ng dL−1) and a PRA <1.0 ng mL−1 h−1 or a PRC lower than the lower limit of the reference range is a positive case detection test result, a finding that warrants further testing (Fig. 1) 11.
Confirmatory tests
With one exception, a high PAC and low PRA test result is not diagnostic by itself, and PA must be confirmed by demonstration of inappropriate aldosterone secretion 11.
The one exception to the requirement for formal confirmatory testing in a patient with hypertension is the clinical setting of spontaneous hypokalaemia with PAC >555 pmol L−1 (>20 ng dL−1) and PRA <1 ng mL−1 h−1 (or PRC below the lower limit of the reference range); this presentation is diagnostic of PA 11.
All other patients should have PA confirmed by demonstration of aldosterone secretory autonomy with aldosterone-suppression testing, which can be performed with orally administered sodium chloride and measurement of urinary aldosterone excretion or with intravenous sodium chloride loading and measurement of PAC 12, 57.
Oral sodium loading test
At Mayo Clinic, we use the oral sodium loading test as our preferred test to confirm PA. Before initiating the high-sodium diet, it is important to normalize serum potassium concentration and achieve hypertension control. Patients should receive a high-sodium diet for 3 days. The goal is a sodium intake of 5000 mg (equivalent to 218 mmol sodium or 12.8 g sodium chloride), an amount that most patients can achieve with dietary changes 13. However, some patients find high-sodium foods unpalatable and may need to supplement their oral sodium intake with sodium chloride tablets. The serum potassium concentration should be monitored daily and oral potassium chloride supplements administered as needed. On the morning of the third day of the high-sodium diet, a 24-h urine collection is started for the measurement of aldosterone, sodium and creatinine. In normal individuals, when the 24-h urinary sodium excretion exceeds 200 mEq there is no reason to release renin or secrete aldosterone. Thus, a urinary aldosterone excretion of more than 33.2 nmol day−1 (>12 μg/24 h) in the setting of low PRA (or PRC) is consistent with autonomous aldosterone secretion 13. The sensitivity and specificity of the oral sodium loading test are 96% and 93%, respectively 58.
Intravenous saline infusion test
The intravenous saline infusion test may also be used to demonstrate aldosterone secretory autonomy 34, 57. Following an overnight fast, 0.9% sodium chloride solution (2 L) is infused intravenously over 4 h with the patient in the seated position 59. Heart rate and blood pressure are monitored during the infusion. At the completion of the infusion, blood is collected for measurement of PAC. PAC levels in normal subjects decrease to less than 139 pmol L−1 (<5 ng dL−1), whereas levels are not suppressed to less than 277 pmol L−1 (<10 ng dL−1) in most patients with PA. Postinfusion PAC values between 139 pmol L−1 (5 ng dL−1) and 277 pmol L−1 (10 ng dL−1) are indeterminate and may be seen in some patients with IHA and less often in patients with APA.
Other confirmatory tests
The fludrocortisone suppression and captopril stimulation tests are less commonly used confirmatory tests. These are described in detail elsewhere 13.
Subtype studies
The optimal treatment of PA depends on whether the aldosterone secretory autonomy is based on one or both adrenal glands. Thus, the goal of subtype testing is to determine whether the source of aldosterone excess is from the right, left or both adrenal glands.
When localized to one adrenal gland (APA or PAH), unilateral adrenalectomy results in normalization of hypokalaemia in all patients; hypertension is improved in all patients and is cured in 30–60% 60–65.
In patients with bilateral adrenal aldosterone hypersecretion (IHA and familial forms of hyperaldosteronism), unilateral adrenalectomy debulks the disease but does not cure the excess aldosterone secretion 13. Thus, IHA and the familial forms of hyperaldosteronism should be treated medically.
APAs are usually small (mean diameter 1.6 cm; <1.0 cm in 16.5% of patients) 65 adrenal nodules with low computed tomography (CT) attenuation [<10 Hounsfield units (HU)] on noncontrast CT and are golden yellow in colour when resected (Fig. 2).
The adrenal glands in patients with IHA may be normal on CT, may show thickening or nodular changes, or may show incidental nonfunctioning adrenal cortical nodules.
When PA is caused by an aldosterone-producing adrenal carcinoma, it is usually characterized by marked biochemical abnormalities (e.g. serum potassium <2.5 mmol L−1), severe hypertension and a unilateral adrenal mass larger than 4 cm in diameter with high noncontrast CT attenuation (e.g. >20 HU) 66.