Today, I review, link to, and excerpt from the Sandra Weintraub, PhD, ABCN/ABPP, FAAN article, Neuropsychological Assessment in Dementia Diagnosis. Continuum (Minneap Minn). 2022 Jun 1; 28(3): 781–799.
doi: 10.1212/CON.0000000000001135. [PubMed Abstract] [Full-Text HTML] [Full-Text PDF].
The above resource has been cited by 5 articles inPubMed.
There are 111 similar articles in PubMed.
All that follows is from the above resource.
KEY POINTS
Abstract
Purpose of review: This article discusses the application of neuropsychological evaluation to the workup of individuals with age-related cognitive impairment and suspected dementia. Referral questions, principles of evaluation, and common instruments to detect abnormalities in cognition and behavior in this population are reviewed. The integration of neuropsychological test findings with other clinical and biomarker information enhances early detection, differential diagnosis, and care planning.
Recent findings: Life expectancy is increasing in the United States, and, accordingly, the prevalence and incidence of dementia associated with age-related neurodegenerative brain disease are rising. Age is the greatest risk factor for the dementia associated with Alzheimer disease, the most common neurodegenerative cause of dementia in people over 65 years of age; other etiologies, such as the class of frontotemporal lobar degenerations, are increasingly recognized in individuals both younger and older than 65 years of age. The clinical dementia diagnosis, unfortunately, is imperfectly related to disease etiology; however, probabilistic relationships can aid in diagnosis. Further, mounting evidence from postmortem brain autopsies points to multiple etiologies. The case examples in this article illustrate how the neuropsychological evaluation increases diagnostic accuracy and, most important, identifies salient cognitive and behavioral symptoms to target for nonpharmacologic intervention and caregiver education and support. Sharing the diagnosis with affected individuals is also discussed with reference to prognosis and severity of illness.
Summary: The clinical neuropsychological examination facilitates early detection of dementia, characterizes the level of severity, defines salient clinical features, aids in differential diagnosis, and points to a pathway for care planning and disease education.
Copyright © 2022 American Academy of Neurology.
INTRODUCTION
In 1976, a seminal article by Robert Katzman1 sent a somber message that foreshadowed the current public health crisis posed by the increasing prevalence of cognitive loss and dementia in later adult years. Before that time, Alzheimer disease (AD), as first reported by Alois Alzheimer, was considered a disease of young onset (ie, a “presenile” dementia), whereas cognitive decline in old age to a point of senility was considered inevitable. In 1968, Blessed and colleagues2 published findings relating postmortem plaque counts to scores on a brief mental status questionnaire. This and other evidence linking Alzheimer neuropathology to cognitive loss argued strongly that dementia should be considered a disease and not a natural or obligatory outcome of the brain aging process.
Katzman’s prophecy has come to pass; it has been estimated that the clinical syndrome of dementia occurs in 6% to 10% of the population older than 65 years of age, two-thirds due to AD pathophysiology.3 As lifespan in the United States and other developed countries increases, and as age constitutes the greatest risk factor for AD and related disorders, a concomitant increase will be seen in the incidence and prevalence of dementia.
AD is not the only neurodegenerative disease that causes dementia, and the past 30 years has seen an increase in our knowledge of these diseases that entail distinct proteinopathies that destroy healthy neurons and their connections. As a result, primary care providers, neurologists, psychiatrists, and other medical specialists will increasingly serve older individuals, many of whom will have mild, moderate, or severe cognitive impairment as the lead symptom or in the background of their primary illness.
So-called normal cognitive aging, although on average portrayed as a steady decline in cognitive test scores can, in fact, be quite heterogeneous, with increased individual variability with advancing age.4 Dementia is the end point of a progressive process during which patients have an initially insidious decline of normal (ie, customary for one’s personal baseline) cognition and/or social-comportmental behavior. The most common cause over age 65 is neurodegenerative brain disease. At postmortem examination, typically one disease (eg, AD) can be identified as a primary finding, but, more often, the primary finding is accompanied by additional types of pathology (eg, limbic Lewy bodies, transactive response DNA-binding protein 43 [TDP-43], or vascular pathology) that are perhaps of lesser magnitude.5
The clinical syndrome of dementia (currently designated as major neurocognitive disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition [DSM-5]6) is defined not only by the presence of cognitive and behavioral decline but also the degree to which this decline interferes with customary functional daily activities. The term neurocognitive was intended to separate neurodegenerative/vascular dementia from other causes of behavioral and cognitive decline that are not specifically linked to a neurologic disease.
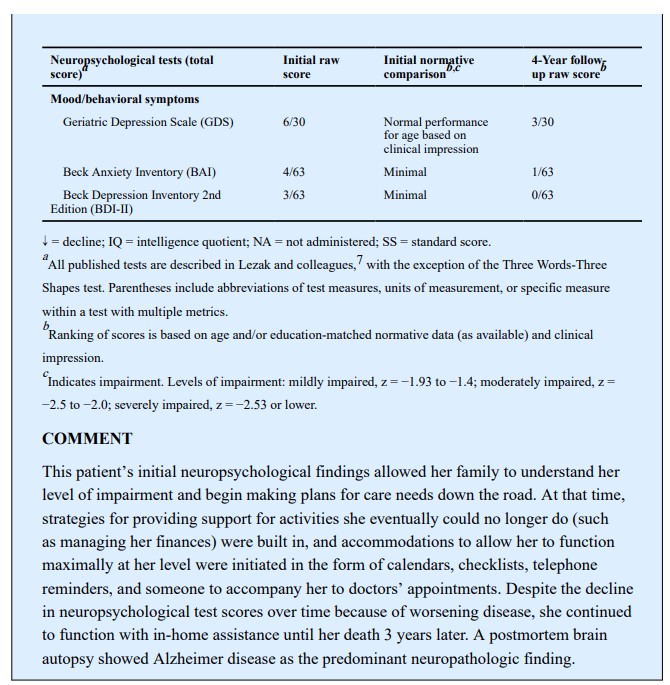
Before dementia, a patient’s cognition and behavior may be changing for many years but not to the extent that prevents an independent existence. During that time, the individual may remain productive and engaged, with appropriate support (Case 6-1).
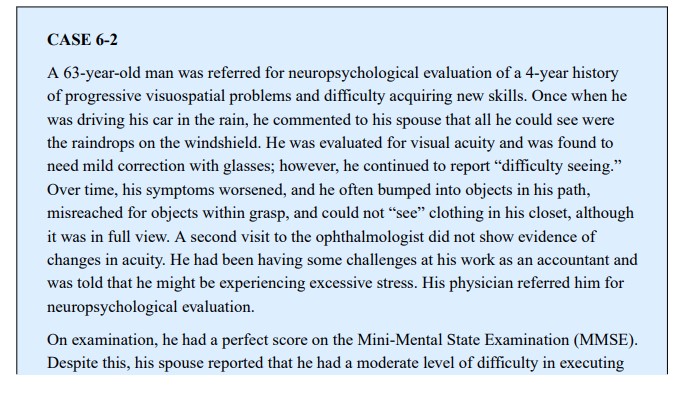
Many dementia syndromes may begin with so-called atypical symptoms that may be attributed to peripheral organ changes (eg, eye problems) (Case 6-2) and misdiagnosed or go unrecognized until further progression occurs.
Although brain autopsy may disclose one predominant neuropathology in an individual with dementia, more often mixed pathologies are detected.5 AD is currently the best studied of the neurodegenerative causes of dementia, likely because of its prevalence; as a result, we now have in vivo biomarkers of its major protein abnormalities (ie, aggregated amyloid and
hyperphosphorylated tau) that can be detected in CSF or by specialized positron emission tomography (PET) scans using tau and amyloid ligands. Less invasive tests for plasma based biomarkers, including neurofilament light chain, amyloid, and phosphorylated tau, are increasingly used predictively13–15 and, when broadly available, will have a significant impact on the diagnostic process. The emergence of amyloid-altering treatments calls for neuropsychological assessment before considering treatment to determine whether an individual has clinical symptoms of AD.Biomarkers notwithstanding, however, increasing concern for dementia is causing individuals to seek evaluation when they subjectively sense a change from their baseline abilities. Interestingly, as cognitive symptoms increase, personal awareness decreases and observer awareness increases.16 In the prodromal or earliest stages of a dementia, especially in those with high prior levels of cognitive achievement and/or education, the routine screening accomplished with such tests as the Mini-Mental State Examination (MMSE),17 the Montreal Cognitive Assessment (MoCA),18 or the cursory bedside clinical
mental status examination may yield no abnormalities. In those cases, it is important not to assume that cognition is normal but rather to escalate to a more rigorous neuropsychological examination. In this case, the neuropsychological examination can detect subtle impairments, identify nonamnestic symptoms that are atypical for dementia onset (eg, simultanagnosia), and, most important, provide a baseline against which longitudinal follow-up examinations can be compared to track progression. If cognitive screening test scores are in the impaired range, neuropsychological testing is also indicated since the examination provides an objective measure of the severity and characteristics of symptoms to use in care planning.19 In the event that the screening score indicates substantial cognitive impairment (eg, 10/30 on the MoCA or 13/30 on the MMSE),
neuropsychological examination is likely to be too challenging for the patient, who in this case would fail on every test, making the detection of a profile impossible. Even in severe
cases, however, the neuropsychologist may choose to administer a brief set of appropriately tailored tests to pinpoint the primary area of deficit (eg, aphasia versus amnesia). In many instances, individuals may no longer be able to remain independent, and several ways to assess safety and decision-making capacity20 are available and can be added to the evaluation as required.Referrals should be preceded by the neurologist’s routine mental status examination, which should include a measure of the ability to learn and retain information after a delay. As noted
above, in individuals with a level of impairment that has significantly affected activities of daily living or in those with scores of less than 18 on the MoCA or MMSE, especially with
a high level of education, the clinician should weigh whether or not the patient would be able to participate in a full neuropsychological battery. A typical battery can take from 2
to 5 hours, depending on the nature of the referral question (eg, a longer evaluation for the question of whether or not a mildly impaired person can continue to work as a financial advisor). Severe cognitive deficits, by screening or as obtained during the interview, would make it difficult to establish the validity/reliability of subsequent extensive testing. Using a brief mental status test can help the neurologist decide whether to refer for further testing, especially in a symptomatic individual, and to narrow the referral question for which additional testing might be useful. A prominent feature of many forms of dementia is a lack of awareness of illness or minimization of symptoms, known as anosognosia. It is important that the patient be accompanied by someone who knows them well enough to provide additional information about changes from past abilities and symptoms. The neuropsychological evaluation will typically obtain information from an informed collateral source, of course, with the patient’s permission. This collateral information may not be available, however, if the patient has no support network or excludes the collateral.THE CLINICAL NEUROPSYCHOLOGICAL EVALUATION
The examination typically begins with a thorough history that includes the patient’s medical conditions; family history of dementia or other medical, psychiatric, or neurologic disease; and concurrent medications. The patient’s level and quality of education and early developmental history are factors that influence the interpretation of neuropsychological test scores and help to determine which weaknesses may have been preexisting. The estimated individual prior peak level of cognitive ability serves as an important guide for the neuropsychologist to select a battery that is appropriate for the individual’s personal academic exposure and career achievements. The neuropsychologist appreciates that even normative standards may not be indiscriminately applied in the case of individuals not educated in the United States, who speak another language, or who have limited education. Thus, appropriate instruments, when available, to test underrepresented groups are critical.25 Also, it is desirable that patients be examined in their preferred language, although a shortage of non–English-speaking neuropsychologists exists in the United States. In this event, the neuropsychologist may work with an interpreter but also must be aware the limitations of this approach.
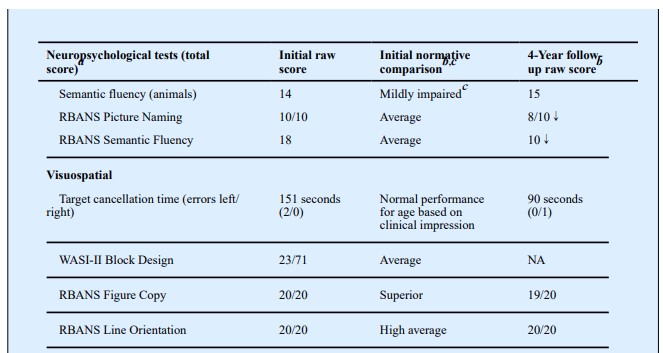
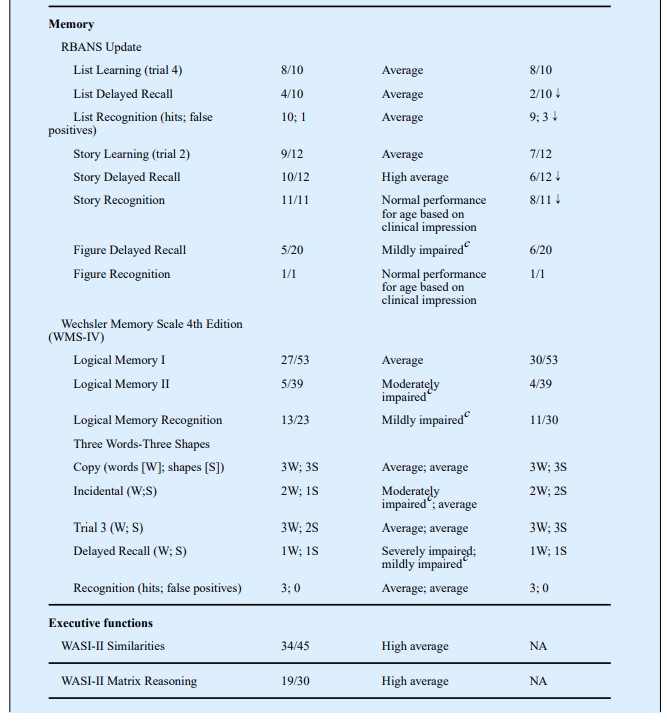
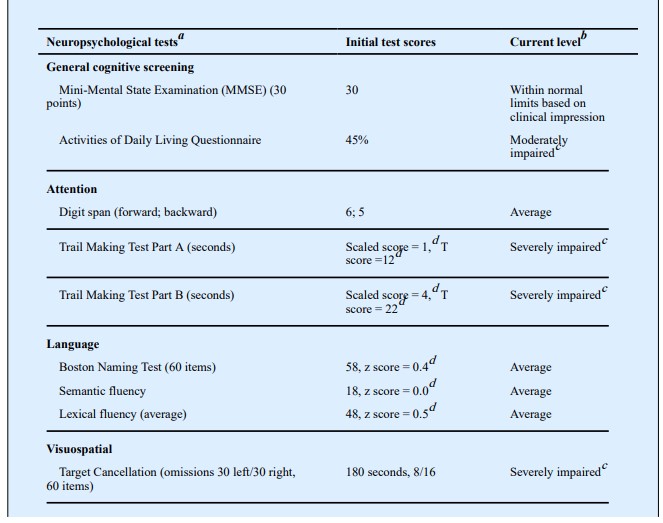
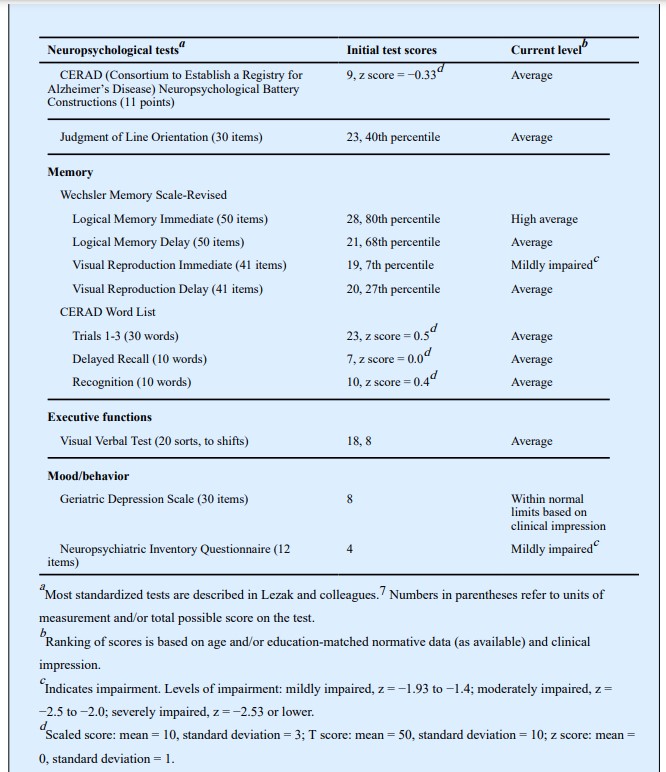
The examination itself consists of objective standardized tests of attention, language, visuospatial perception, episodic memory, and executive functions (Table 6-126). Each of these domains has been well studied in terms of the brain networks underlying them and how they are disrupted by neurologic disease. The scores obtained are compared with normative standards for the patient’s age, level of education, and other relevant demographics so that the level of functioning in each domain and the degree to which it diverges from expectation can be quantified. Social cognition, also referred to as comportment or social-interpersonal skill, is commonly assessed through informant interview and, in some cases, by objective measures.27 In addition to weighing the impact of education and experience on test performance, the neuropsychologist must also consider whether medications or extant medical conditions could be contributing to test performance.
Some common scenarios for considering referral for neuropsychological evaluation include the following:
History Taking
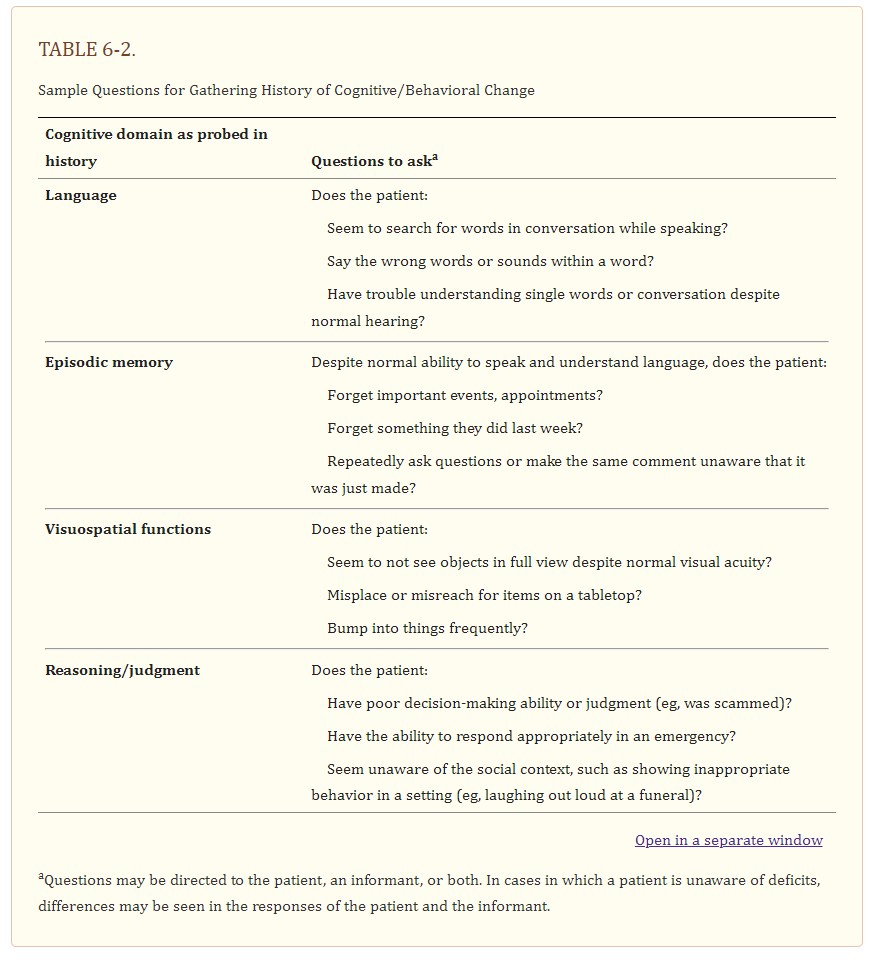
The neuropsychologist probes for evidence of a change from a person’s prior level of cognitive ability, character, and/or emotions and behavior. This is typically difficult to obtain because patients often do not recognize the changes. Even those who observe them may not accurately time the onset of symptoms, becoming aware of them only after a crisis. It is important to ask when patients last seemed like themselves in terms of carrying out routine activities, interacting with others, making decisions, and displaying typical emotional reactions (eg, sympathy, empathy). The key to detecting a dementia syndrome is change, not the specific symptom itself. Most individuals report a variety of cognitive symptoms as “memory loss.” Deeper probing can determine the neurocognitive domain within which the symptom really falls. For example, individuals with aphasia may report forgetting words, individuals with visuospatial deficits may report forgetting how to use common tools, and individuals with behavioral changes may report forgetting their manners. Table 6-2 lists some questions to use in history taking to elicit distinctive symptoms in a framework that is neurologically relevant for cognitive-behavioral neuroanatomic networks.
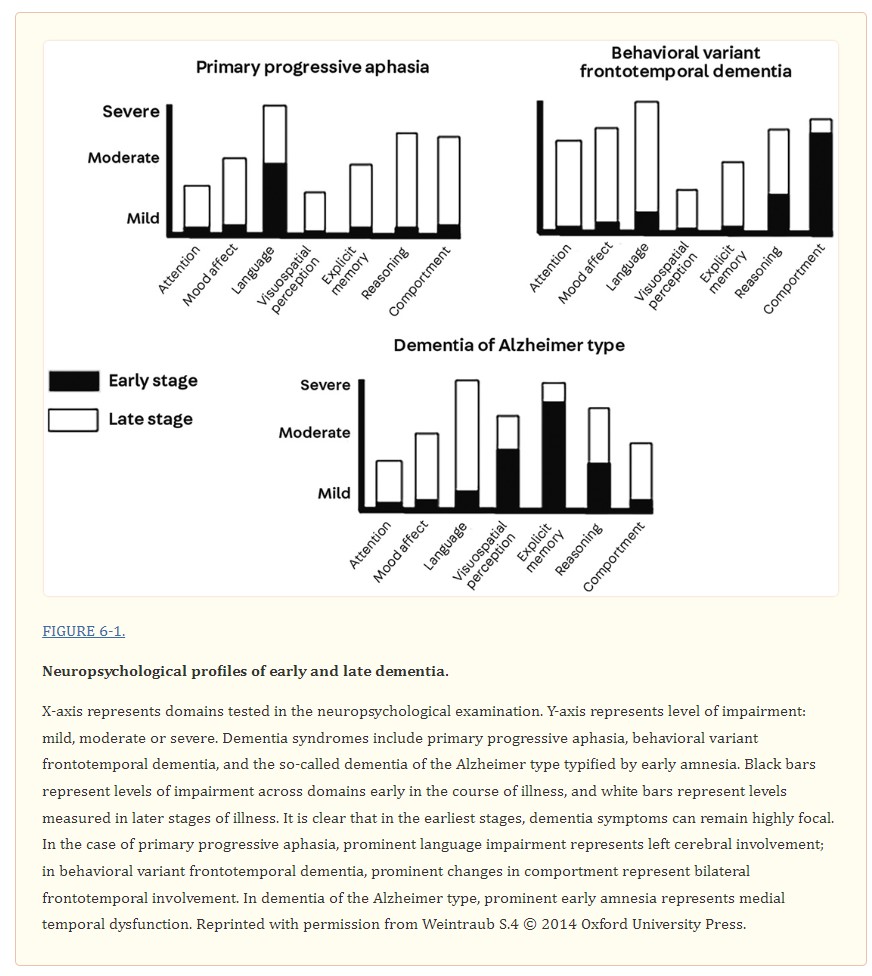
The cognitive and behavioral functions surveyed in the examination are based on a model that relates complex cognitive functions to their underlying neuroanatomic and functional brain networks. Symptoms in domains such as language, spatial perception, visual object perception, social cognition, and episodic memory lend themselves to neuroanatomic network localization, whereas symptoms such as reduced arousal and attention are not easily localized in the same manner.8 The goal of the neuropsychological examination of an individual with suspected dementia, especially in the early stages, is to identify whether a single domain is involved (eg, episodic memory versus aphasia) or whether the patient has multiple cognitive and behavioral deficits. The early clinical profile (Figure 6-1) reflects the areas of the brain influenced by disease rather than the disease itself. Thus, aphasia as a predominant early symptom implies left-sided cerebral involvement in most right-handers and half of left-handers, whereas amnesia implies damage to medial temporal limbic areas.
The neuropsychological examination reviews attention, episodic memory, language, visuospatial functions, and executive abilities such as reasoning and set shifting. The interpretation takes into account how deficits in one domain can affect scores on tests in another domain, although that domain itself may be intact. For example, to establish that episodic memory is intact in the patient with word-finding difficulty, tests that will not be affected by the aphasia have to be used. The Three Words–Three Shapes Test was designed to compare verbal and nonverbal memory in the visual modality; the test can distinguish among different clinical dementia syndromes such as amnestic dementia (in which memory loss is paramount) and primary progressive aphasia (in which patterns of performance reflect the integrity of nonverbal episodic memory and recognition of verbal information that may not be retrievable spontaneously).29,30
Biomarkers have clearly been an advance in diagnosis, at least for AD. However, biomarkers do not provide information about the specific cognitive and behavioral symptoms an individual is experiencing, and these symptoms are not homogeneous across individuals with AD or other neurodegenerative diseases. Symptoms can differ vastly and need different interventions.
A BLUEPRINT FOR EDUCATION, SYMPTOM MANAGEMENT, AND MONITORING
The results of the neuropsychological examination are shared with the patient and support network as available, usually in the form of an in-person feedback session. During this session, the neuropsychologist reviews the findings and translates what they mean in terms of the individual’s experience, impact on daily living, and significance for diagnosis. It is important to explain the limits of knowledge based on the examination, that is, that the neuropsychological examination detects whether cognition or behavior is abnormal and specifies which functions are not normal but does not identify the disease causing the abnormality.
CONCLUSION
Cognitive aging is heterogeneous, and not all decline is benign. With increasing recognition that age-related cognitive decline could imply future dementia, it is important for neurologists to obtain an objective measure of a patient’s cognitive function to inform the diagnosis, prognosis, and care recommendations. The clinical neuropsychological examination addresses issues that are not easily assessed in the cursory mental status examination or obtained in routine imaging and laboratory tests:
The neuropsychological examination can also document normal mental state in an individual with cognitive symptoms and then serve as a baseline against which future changes can be measured.