See also ACG Clinical Guideline: Evaluation of Abnormal Liver Chemistries [PubMed Abstract] [Full-Text HTML] [Download Full-Text PDF]. Am J Gastroenterol. 2017 Jan;112(1):18-35. doi: 10.1038/ajg.2016.517. Epub 2016 Dec 20.
Here are the recommendations from the above resource:
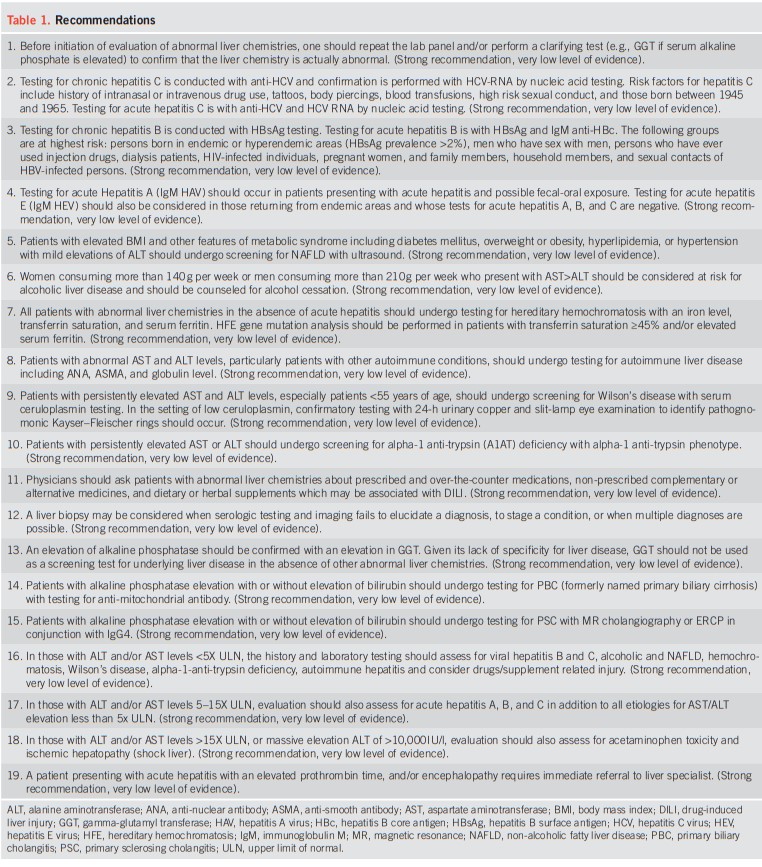
And see my summary post: Reposting Excerpts From The 2017 Guidelines On The Evaluation Of Abnormal Liver Tests From The ACG
Posted on February 14, 2023 by Tom Wade MD
Today, I review, link to, and excerpt from The Curbsiders’ #293 The Best of Liver Tests with Dr. Elliot Tapper*.
*Gibson EG, Tapper EB, Williams PN, Watto MF. “#293 The Best of Liver Tests with Elliot Tapper”. The Curbsiders Internal Medicine Podcast. http://thecurbsiders.com/episode-list Final publishing date September 6, 2021.
All that follows is from the above resource.
Embed #293 when connected.
Take a walk through Liver Land with Dr. Elliot Tapper (@ebtapper on Twitter) as we stroll through the best of liver tests. Once differentiating a hepatocellular versus cholestatic injury picture, Dr. Tapper shares some targeted labs to help with etiology, as well as what to do with those pesky isolated lab abnormalities. On top of that, we review common causes of severe acute liver disease and issues in pregnancy. Join us, and you’ll be writing more accurate notes as Dr. Tapper schools us on what “liver function tests” really mean!
Show Segments
- Intro, disclaimer, guest bio
- Guest one-liner
- Definitions of liver enzymes, liver function tests
- Patterns of acute liver injury
- Drug-induced liver injury
- Isolated alkaline phosphatase elevation
- Isolated total bilirubin elevation
- Livery Injury During Pregnancy
- Acute liver failure
- Outro
The Best of Liver Tests Pearls
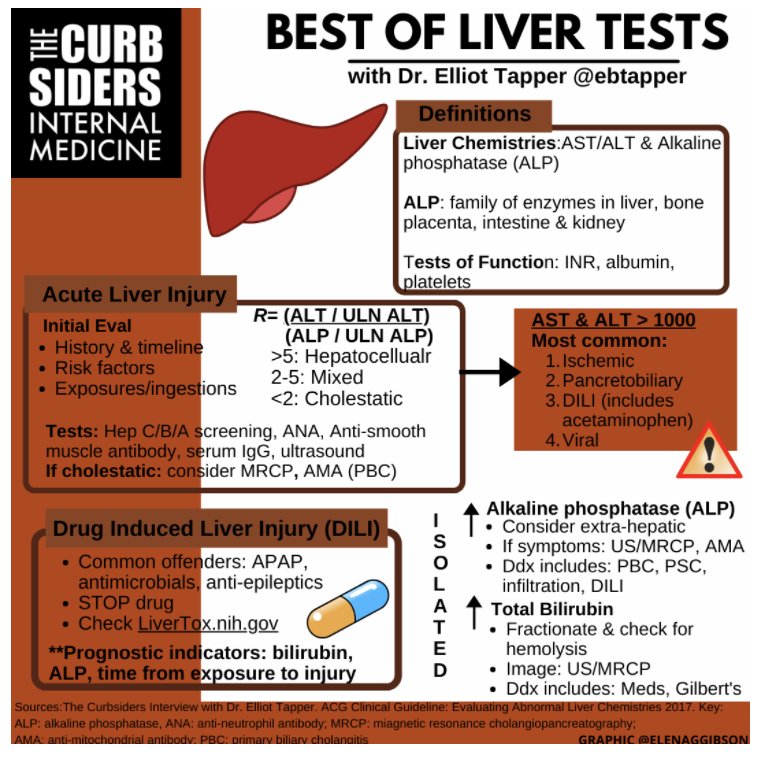
- Elevations in the liver enzymes ALT and AST suggest hepatocyte injury while an elevation in alkaline phosphatase suggests injury to the bile duct.
- Tests of liver function include albumin, the INR, platelets and bilirubin.
- The R score can be used to differentiate hepatocellular and cholestatic patterns of acute liver injury. An R ratio >5= hepatocellular injury, <2=cholestatic, and 2-5=mixed.
- The degree of bilirubin elevation is the most important prognostic factor in DILI.
- The labs used to evaluate for autoimmune hepatitis include: ANA, anti-smooth muscle antibody (or F-actin) and serum IgG.
- Initial lab evaluation for acute hepatocellular injury should include: Hepatitis A/B/C testing, autoimmune hepatitis testing (see above), acetaminophen levels if severe.
- Hemochromatosis and alpha-1-antitrypsin do not usually present with acute enzyme elevations, so testing is not necessary for acute injury. Wilson’s disease is rare, especially in older adults.
- Three main causes of liver disease in pregnancy include: 1) non-pregnancy related causes 2) preeclampsia 3) intrahepatic cholestasis of pregnancy.
- The most common etiologies of severe liver injury with an AST & ALT >1000 IU/L in the United States include: 1) ischemic hepatitis 2) pancreatobiliary sources 3) DILI and 4) viral hepatitis.
- Acute liver failure is defined by severe acute liver injury plus significant coagulopathy (INR >1.5) and hepatic encephalopathy.
The Best of Liver Tests Notes
Liver Tests
Liver chemistries include the enzymes of serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and alkaline phosphatase. These are markers of liver injury, not liver function!
Tests of liver function include the INR/prothrombin time, bilirubin, albumin and platelets. Albumin is a marker of longer term liver function as it is synthesized by the liver and has a half-life of 3 weeks (ACG Guideline 2017). Dr. Tapper also introduces a variety of tests that more closely evaluate hepatic metabolism including:
- 13-C Methionine breath test (Braden 2007)
- Ammonia clearance test by Shelia Sherlock (Shelia AASLD Obituary)- not recommended!
- Caffeine clearance test
Alkaline phosphatase & gamma-glutamyl transferase (GGT): alkaline phosphatase is a family of enzymes that are found in hepatocytes, bone, placenta, intestine and kidney. GGT is often suggested as a way to determine if alkaline phosphatase is coming from the liver, but Dr. Tapper describes how this is not always as helpful in clinical practice because GGT is “not specific for any one liver disease or even the liver itself” (Twitter thread by @ebtapper).
Pattern of Injury
If it is not clear, the R score or ratio can be used to assess for a hepatocellular, cholestatic or mixed pattern of liver injury. The R ratio is equal to the patient’s ALT divided by the upper limit of normal (ULN) for the ALT over the patient’s alkaline phosphatase divided by the ULN for alkaline phosphatase. An R ratio >5= hepatocellular injury, <2=cholestatic, and 2-5=mixed (ACG Guideline 2017).
R= (ALT value / ALT ULN) / (alk phos/ alk phos ULN)
Dr. Tapper explains how the ratio of AST to ALT of 2:1 in alcohol related hepatitis is often taught but is not very sensitive or specific, particularly once the aminotransferase values are >1000. However, the degree of elevation in aminotransferases is helpful. Furthermore, if the (AST + ALT) > 500 the likelihood of the injury being caused by alcohol alone is low.
Hepatocellular injury: Common etiologies include drug-induced liver injury, autoimmune hepatitis and viral hepatitis. In hospitalized or very ill patients, consider ischemic hepatitis (often termed “shock liver”) or drug induced injury from acetaminophen.
Labs: check hepatitis A, hepatitis C, hepatitis B in most cases. If a transplant patient or recent chemotherapy consider CMV or other herpes virus. Test significant hepatitis for autoimmune hepatitis with an ANA, anti-smooth muscle antibody and IgG. Testing for hemochromatosis with an iron panel or for alpha-1-antitrypsin deficiency may be considered for chronic liver disease, but would not diagnose a new, acute injury. Similarly, most people do not have an indication for testing for Wilson’s disease initially which is rare and occurs more in children and younger adults.
Imaging: if liver injury, particularly if abdominal symptoms, get an ultrasound. If the index of suspicion is high for choledocholitiasis or you don’t have another source, consider cross-sectional imaging with MRCP.
Cholestatic injury: Common causes are biliary obstruction, primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), sarcoidosis, common variable immunodeficiency (CVID), and DILI.
Labs: ANA, anti-smooth muscle antibody, IgG, anti-mitochondrial antibody (for PBC)
Imaging: ultrasound or MRCP to evaluate for biliary obstruction
Autoimmune Hepatitis
These patients will often present with a strongly positive ANA, smooth muscle antibody (>1:80), and an elevated serum IgG several fold higher than the upper limit of normal. Note some labs may report F-actin by direct antigen testing, which is another lab technique that correlates with the titer of smooth muscle antibody tests. Consider referring these patients for a liver biopsy to determine diagnosis and need for immunosuppression. Note that drugs (like nitrofurantoin or minocycline) may trigger autoimmune hepatitis or present with a similar pattern of liver injury.
Drug-induced Liver Injury (DILI)
DILI is broadly defined as abnormalities in liver tests following introduction or continued use of a drug with other etiologies of liver injury excluded. Liver injury that occurs in a medication with a history of causing DILI should raise your suspicion. Dr. Tapper recommends LiverTox as a resource for information on prior reports of DILI with a specific drug exposure. DILI can also present with an autoimmune hepatitis picture, as above. The prognosis for DILI is worsened by an increased alkaline phosphatase elevation, bilirubin elevation, and prolonged time from ingestion of the drug to presentation with liver injury (Ashby 2021). Dr. Tapper usually follows stable patients regularly with labs until improvement or opts for a liver biopsy if concerned.
Isolated Lab Abnormalities
Alkaline phosphatase elevations
Elevations in alkaline phosphatase with symptoms such as pruritus should prompt additional workup with imaging (ultrasound first then consider MRCP). The differential for the etiology of includes biliary obstruction, infiltrative disease (including malignancy), primary biliary conditions (PBC or PSC), sarcoidosis, CVID, and DILI.
Bilirubin elevations
First, fractionate the total bilirubin. If >50% is direct= direct hyperbilirubinemia. Otherwise=indirect bilirubinemia. Usually with indirect hyperbilirubinemia 80-90% of bilirubin will be indirect. For indirect hyperbilirubinemia, check LDH, haptoglobin and reticulocyte count to evaluate for hemolysis. If there is no hemolysis, the diagnosis of Gilbert’s can be made. Usually, the total bilirubin in Gilbert’s disease will be <4mg/dL but certain factors including fasting, sleep deprivation and smoking can lead to further elevations due to decreased function of the remaining uridine-5′-disphosphate gluconyltransferase 1A1 (UGT1A1) (Shroff 2020).
Pregnancy
Three main causes of liver disease in pregnancy: 1) non-pregnancy related causes 2) preeclampsia 3) intrahepatic cholestasis of pregnancy. About 1/3 of elevated liver enzymes in patients with pregnancy are intrahepatic cholestasis of pregnancy. Patients will usually present with pruritus, elevated alkaline phosphatase and an elevated serum bile salts level (Marschall 2019). It is important to trend and treat serum bile salt levels because the elevation in bile salts is related to outcomes in pregnancy (Ovadia 2019). The elevation in bile salts is related to outcomes in pregnancy with a level >40μmol/L associated with non-lethal adverse outcomes and > 100 μmol/L associated with stillbirth (Marschall 2019). Ursodiol and cholestyramine can be used for management, and repeat bile salt monitoring will be used to determine when to deliver.
Severe Acute Liver Injury and Acute Liver Failure
In the United States, most causes of an AST and/or ALT > 1000 IU/L (severe acute liver injury) are ischemic hepatitis, choledocholithiasis, DILI and acute viral hepatitis (Breu 2019). Ischemic hepatitis can occur in normotensive patients and generally occurs in persons with severe hepatic congestion or right heart failure. Acute liver failure is defined by a severe acute liver injury PLUS a significant coagulopathy (INR >1.5) AND hepatic encephalopathy (Bernal 2013). Acute liver failure is a very rare subset of acute liver injury usually caused by drugs (acetaminophen, antiepileptics, antimicrobials) or acute viral hepatitis.