
The first excerpts are from Dr. Horeczko’s podcast podcast Pediatric Headache: Some Relief for All Updated on September 1, 2016 of The Pediatric Emergency Playbook.
The second set of excerpts are from Migraine Cocktail of from Pediatric EM Morsels
BY DR SEAN FOX · PUBLISHED FEBRUARY 5, 2015 · UPDATED FEBRUARY 11, 2015
The following are excerpts from the show notes of Dr. Horeczk0’s outstanding podcast Pediatric Headache: Some Relief for All Updated on September 1, 2016 of The Pediatric Emergency Playbook:
Primary or Secondary?
Primary headaches: headaches with no sinister secondary cause – like tension or migraine – are of course diagnoses of exclusion (cluster headache is exceedingly rare in children).
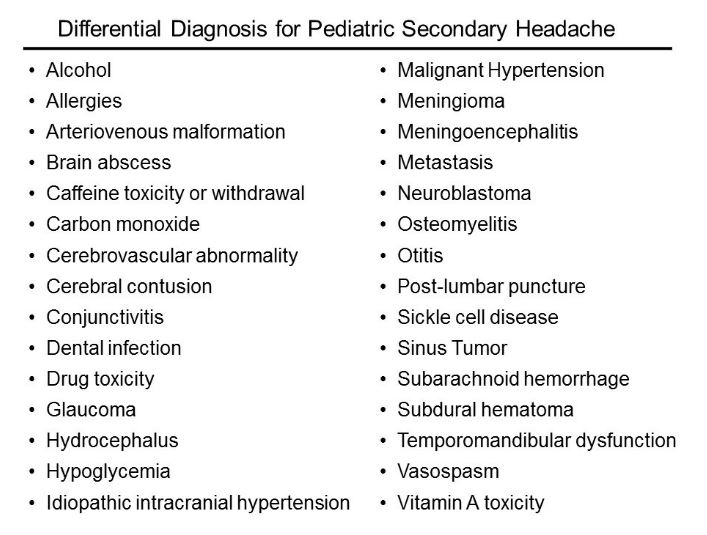
Secondary headaches: headaches due to some underlying cause – are what we need to focus on first [maybe it is something bad].Secondary Headache?
Is it a tumor?
Is it an infection?
Is it a bleed?
Who needs neuroimaging?
The short answer is, if the child has an abnormal exam finding, then obtain a non-contrast head CT in the ED. If you’re worried enough to get imaging, then you should not feel great about sending him to an expedition to MRI.
The reassuring point is that for a child with a normal neuro exam, we have time to figure this out. For the recurrent headache, outpatient MRI really is the way to go if at all possible – not only do we forgo unnecessary radiation, but MRI is more likely to reveal the cause – or rule out the concern.Other Causes of Secondary Headaches:
Primary Headache Management
So how do we treat primary headaches? If you feel this is a mild tension headache, fluids by mouth and a simple NSAID are probably all that is needed, in addition to a heaping dose of reassurance. Ibuprofen (10 mg/kg/dose q 6h, up to 600 mg) for a short course has the most evidence basis. Acetaminophen (paracetamol) (15 mg/kg/dose q6 h) for a short course may also be given.
Abortive treatments with the triptans may have been tried at home, but if they are coming to see us, we are past the point where triptans will be helpful.For the primary headache that is resistant to NSAIDs, IV therapy may be considered.
If you’re going for IV, a nice evidence-based migraine cocktail is the following:
1. A bolus of 20 ml/kg of normal saline, up to a liter
2. Ketorolac (0.5 mg/kg; max, 30 mg)
3. Diphenhydramine (1 mg/kg; max, 50 mg)
4. Prochlorperazine (0.1 mg/kg; max, 10 mg)
The following is from Migraine Cocktail of from Pediatric EM Morsels
BY DR SEAN FOX · PUBLISHED FEBRUARY 5, 2015 · UPDATED FEBRUARY 11, 2015:
Pediatric Migraine
Headaches are common in the ED
2-3% of ED for all ages.
Account for ~1% of Ped ED visits
Most headaches are due to benign causes.Prevalence of Pediatric Migraine
Difficult to know true prevalence.
Increases with age:
3-7 yrs: 1-3%
7-11yrs: 4-11%
by 15yrs: 8-23%
Typically have had 2-3 days of headache prior to ED presentation.
Often (>60%) have already tried abortive therapies. [Richer, 2010]
Most are able to be treated effectively in the ED and discharged to home. [Bachur, 2015]Migraine Therapies for Kids
Ibuprofen
Effective and safe [Evers, 2006; Lewis, 2002]
Considered by many to be first line therapy, but often used by patient prior to arrival in ED.Triptans
NOT FDA approved for use in children, and are used “off label.”
Evidence that NSAID is equally efficacious.
Sumatriptan nasal spray has been shown to be safe and efficacious for adolescents. [Lewis, 2004; Winner, 2000]
Combination of Sumatriptan with NSAID has shown to be effective in adolescents also. [Derosier, 2012]
No ED-Based studies of use of triptans for children available yet.Prochlorperazine
Shown to be more effective than IV NSAID (my least favorite NSAID). [Brousseau, 2004]
Recent publication showed that prochlorperazine use was associated with lower rate of return ED visits compared to metoclopramide (certainly not causal relationship). [Bachur, 2015]
Often administered with diphenhydramine to prevent akathisia, although also found to be associated with higher return ED visit rates. [Bachur, 2015]Migraine Approach (in my humble opinion)
Do a thorough neuro exam!
Channel your inner neurologist.
Documenting a truly normal neuro exam goes a long way toward defining this headache as a benign one.
Do a Fundoscopic exam!
Again, let us make sure we are not missing pseudotumor… or a real tumor.
A PanOptic Ophthalmoscope is much easier to use on kids!
Headaches suck… don’t be dismissive.
After you have decided that this is a benign headache, realize that the kid doesn’t think it is benign.Try a Triptan
If the patient is an adolescent, this is a reasonable option.
One Migraine Cocktail Coming Up.
There appears to be some evidence to favor Prochlorperazine over metoclopramide.
Keep diphenhydramine handy… remember that you should first do no harm.



