
Dr. Scott Weingart of the EmCrit Podcast has just posted Podcast 181 – Pulmonary Hypertension and Right Ventricular Failure with Dr. Susan Wilcox [link is to the shownotes and podcast].
Be sure to review Dr. Josh Farkas’ outstanding thoughts about intubating the crashing pulmonary hypertension patient in the emcrit podcast shownotes. Always review the thoughful reader comments that accompany each of Dr. Weingart’s podcasts.
The following are excerpts from the shownotes:
Intubating patients with Acute RV failure: Very high risk [So be very sure the patient needs it]
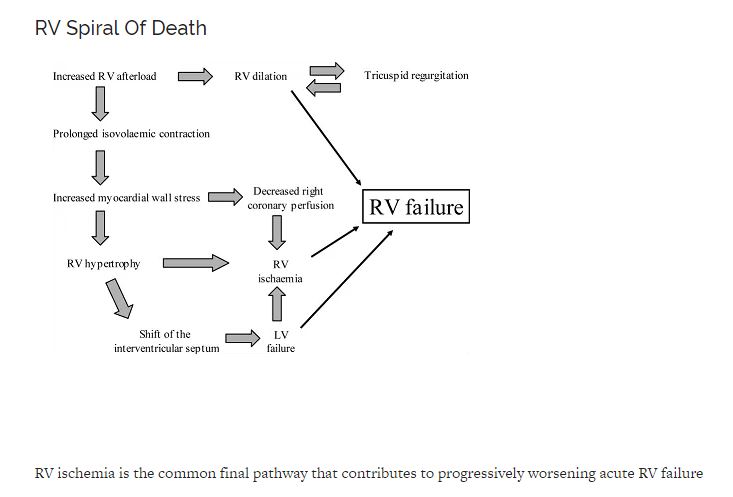
- Intubation with RSI = Loss of native catecholamines leading to vasodilation and decreased venous return/preload leading to RV cardiac output to worsening RV ischemia to worsening RV failure
- Intubation with inadequate sedation leads to pain and agitation with airway manipulation leading to increased intrathoracic pressure and increased PVR to decreased venous return/preload leading to in RV cardiac output leading to worsening RV ischemia leading to worsening RV failure
- Strongly consider fentanyl, ketamine awake intubation
How to Do it
- PREPARE and GET HELP
- If urgent/semi-emergent intubation
- Place arterial line, obtain good vascular access
- Optimize volume status
- Consider awake intubation or awake fiberoptic intubation
- May help minimize hemodynamic perturbation
- Use topical lido + small dose of safe sedative
- Utilize video laryngoscopy
- Most experienced intubator
- If emergent intubation
- RSI with etomidate
- Anticipate hemodynamic collapse – use push-dose epinephrine, have norepinephrine or epinephrine drip already hanging
- I will “premedicate” pts with RV failure with push dose of 10-20mcg of epinephrine and 1-2U of vasopressin just prior to induction even if they aren’t hypotensive
- Re-evaluate volume status following intubation
ECHO: How to evaluate for RV failure at bedside
- Apical 4 chamber to evaluate relative size of RV to LV and to evaluate how RV “looks”
- If you are skilled, focus on lateral tricuspid annulus movement (TAPSE) 1.6
- McConnell’s sign may be indicative of acute RV failure with RV ischemia, not just seen in acute PE
- Parasternal short at level of mid-papillary to eval relationship between volumes and size of LV and RV and intraventricular septum – look for septal shift and the “D” Sign
- Plethoric IVC regardless of volume Status
- As RV dilates in chronic failure, there will be disruption of the tricuspid annulus leading to tricuspid regurg
Please go to the podcast 181 snowshoes for the “Six Step Approach to Management of Acute RV Failure.
Additional Resources
[All the following except for Tutorial 7 are from Dr. Weingart’s EmCrit Podcast 181 – Pulmonary Hypertension and Right Ventricular Failure with Dr. Susan Wilcox]. Be sure to review Dr. Josh Farkas’ outstanding thoughts about intubating the crashing pulmonary hypertension patient in the emcrit podcast shownotes. Always review the thoughful reader comments that accompany each of Dr. Weingart’s podcasts.
Tutorial 7 – Assessment of the right heart from criticalecho.com – ICU Sonography:
Demystifying sonology in intensive care
Playford on pulmonary hypertension podcast from The Intensive Care Network.
Pulmonary Hypertension and Right Ventricular Failure in Emergency Medicine [PubMed Abstract] [Full Text PDF]. Ann Emerg Med. 2015 Dec;66(6):619-28. doi: 10.1016/j.annemergmed.2015.07.525. Epub 2015 Sep 3.
Intensive care unit management of patients with severe pulmonary hypertension and right heart failure [PubMed Abstract] [Full Text PDF]. Am J Respir Crit Care Med. 2011 Nov 15;184(10):1114-24. doi: 10.1164/rccm.201104-0662CI.
Acute Right Ventricular Failure in the Setting of Acute Pulmonary
Embolism or Chronic Pulmonary Hypertension: A Detailed Review of the
Pathophysiology, Diagnosis, and Management [PubMed Abstract] [Full Text HTML] [Full Text PDF]



