In this post, I again review, link to, and excerpt from The Curbsiders‘ [Link is to the complete list of episodes] episode #308 Metabolic Alkalosis and Hypokalemia: Kidney Boy Returns!. By
All that follows is from the above outstanding podcast shownotes.
@Kidney_Boy returns to school us on metabolic alkalosis and hypokalemia! What do diuretics, hyperaldosteronism, black licorice, and milk-alkali have in common? Our Chief of Nephrology, Dr. Joel Topf, talks through the pathophysiology of metabolic alkalosis, the utility of urine chloride and pH measurements, why normal saline is sometimes better than balanced solutions, when to reach for acetazolamide, and more! Urine for a good time ; )
Metabolic Alkalosis and Hypokalemia Pearls
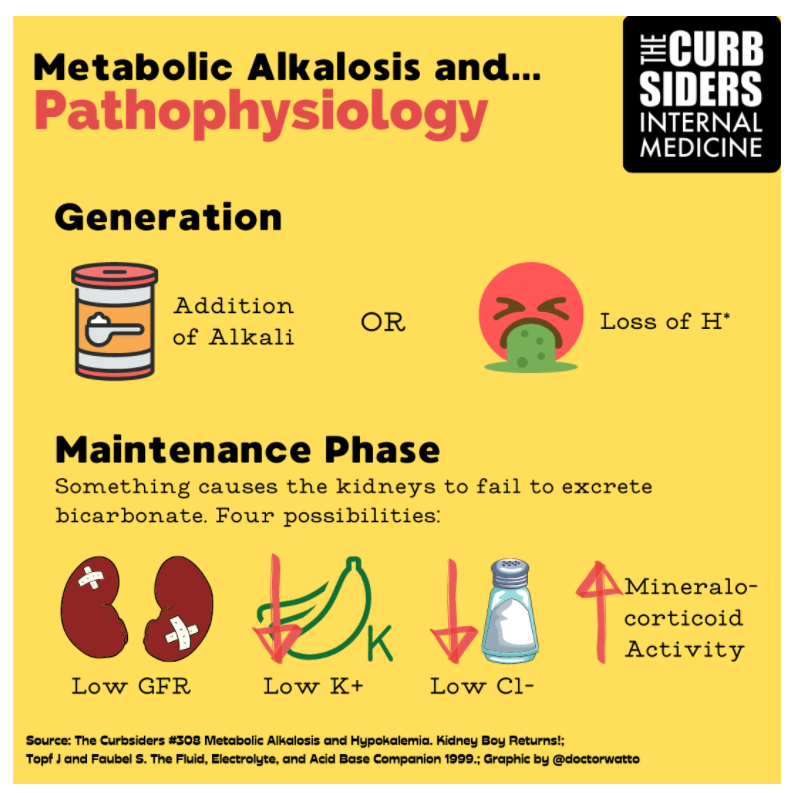
- When approaching the diagnosis (or etiology) of metabolic alkalosis divide it into Generation and Maintenance.
- Generation of metabolic alkalosis is the addition of alkali (taking calcium carbonate pills, eating baking soda) or the loss of hydrogen ions (vomiting, diuretics).
- Maintenance of metabolic alkalosis is what is wrong with the kidney that prevents it from just excreting the excess bicarbonate. There are four causes for the maintenance of metabolic alkalosis
- Decreased GFR (kidney failure)
- Decreased chloride (hypovolemia)
- Hypokalemia
- Increased mineralocorticoid activity
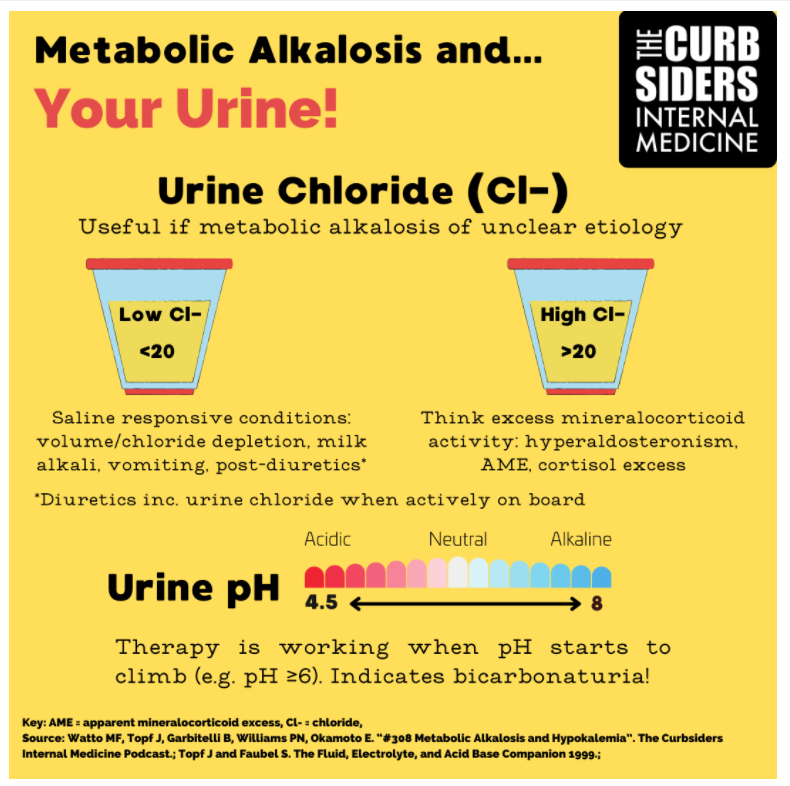
- Low urine chloride suggests a chloride responsive metabolic alkalosis (milk alkali, volume depletion, vomiting, diuretics) and high urine chloride suggests mineralocorticoid excess.
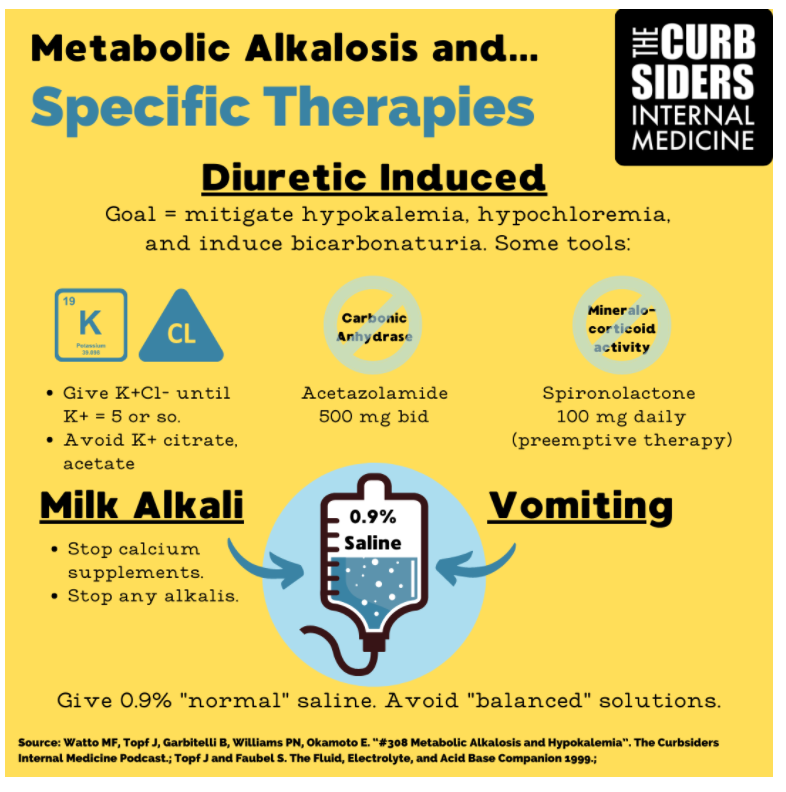
- Use normal saline instead of a “balanced” IV fluid (e.g. lactated ringers) for the patient with metabolic alkalosis from vomiting.
- A teaspoon of baking soda has 60 mEq of bicarb while a 650 mg bicarb pill has only 8 mEq. Thus, patients with renal insufficiency or volume depletion who consume baking soda can get into trouble.
- Give potassium chloride at escalating doses in patients undergoing diuresis to prevent/treat hypokalemia, hypochloremia. Avoid potassium acetate or potassium citrate which are both alkalis!
- Consider acetazolamide 500 mg twice daily to help lower the bicarb and monitor the urine pH, which will increase when the drug starts working.
- High-dose spironolactone (e.g. 100 mg/day) can help prevent hypokalemic metabolic alkalosis during diuresis for heart failure exacerbation.
- Follow the urine pH during treatment of metabolic alkalosis to detect bicarbonaturia (a marker of treatment success!).
The Rodney Dangerfield of Electrolyte Disorders
Metabolic alkalosis is the most common disorder seen on a blood gas in hospitalized patients (Hodgkin, 1980). Dr. Topf says, “Metabolic alkalosis is the Rodney Dangerfield of electrolyte disturbances”. A big reason is because severe clinical consequences like seizures are uncommon (Emmett, UpToDate 2021). Symptoms can often be attributed to associated electrolyte disturbances, namely hypokalemia (Emmett, UpToDate 2021).
Pathophysiology of Metabolic Alkalosis
Dr. Topf notes that under normal circumstances the proximal tubule reabsorbs thousands of mEq of bicarbonate each day (Emmett, 2020). Therefore, to correct metabolic alkalosis it just needs to work less and let that bicarb “pour out of the kidney”.
Metabolic alkalosis is generated by the addition of alkali (e.g. bicarbonate), volume depletion, or the loss of hydrogen ions (Topf, Fluid Electrolyte and Acid Base Companion, 1999). It’s maintained by inability of the kidneys to excrete bicarbonate. As Dr. Topf puts it, “something paralyzes the kidney and forces it to reabsorb bicarb against its will”. Potential mechanisms include excess alkali intake with a low GFR (acute or chronic failure), volume depletion/chloride deficiency, hypokalemia (intracellular acidosis fools the kidney into retaining bicarbonate), and increased mineralocorticoid activity (due to volume depletion, primary hyperaldosteronism, Cushing’s syndrome) —Topf, Fluid Electrolyte and Acid Base Companion, 1999.
Metabolic Alkalosis from Vomiting
Use saline to correct volume and restore chloride levels (Metha, UpToDate 2021, Emmett, 2020). Don’t choose a “balanced” IV fluid (e.g. lactated ringers) for the patient with metabolic alkalosis from vomiting. Dr. Topf cautions, “This patient is starving for chloride and sodium so normal saline is the fluid of choice in this situation.” Technically, the diagnosis requires a blood gas, but this presentation is so classic that it would be reasonable to avoid the extra stick (expert opinion).
Kashlak Pearl – When someone develops a metabolic alkalosis from vomiting they begin to excrete the excess bicarbonate in their urine. This acts like a magnet for potassium and causes increased renal excretion.
Metabolic Alkalosis from Vomiting
Use saline to correct volume and restore chloride levels (Metha, UpToDate 2021, Emmett, 2020). Don’t choose a “balanced” IV fluid (e.g. lactated ringers) for the patient with metabolic alkalosis from vomiting. Dr. Topf cautions, “This patient is starving for chloride and sodium so normal saline is the fluid of choice in this situation.” Technically, the diagnosis requires a blood gas, but this presentation is so classic that it would be reasonable to avoid the extra stick (expert opinion).
Kashlak Pearl – When someone develops a metabolic alkalosis from vomiting they begin to excrete the excess bicarbonate in their urine. This acts like a magnet for potassium and causes increased renal excretion.
Baking Soda and Metabolic Alkalosis
Kashlak Pearl – A baking soda teaspoon has 60 mEq of bicarb while a 650 mg bicarb pill has only 8 mEq. Thus, patients with renal insufficiency or volume depletion who consume baking soda can get into trouble.
Kashlak Pearl – Baking soda is a major component of crack cocaine and thus patients receive high doses of bicarb. This can cause profound metabolic alkalosis for patients with advanced renal disease who cannot excrete bicarb on their own. Case reports exist (Diskin, 2006).
Potassium supplementation
Dr. Topf recommends giving potassium chloride at slowly escalating doses until the potassium hits 5 or above to prevent/treat hypokalemia, hypochloremia, and provide a buffer during diuresis (expert opinion). Further, this gradual increase in potassium chloride supplementation allows us to correct the chloride without giving normal saline, and without potassium reaching dangerous levels (expert opinion).
Kashlak Pearl – Don’t give potassium acetate because acetate will be converted to bicarbonate in the liver (see Pfizer package insert), which can potentiate metabolic alkalosis. Similarly, potassium citrate is also an alkali.
Kashlak Pearl – Dr. Topf notes that patients with metabolic alkalosis from diuretics have acidic urine pH (e.g. pH of 6 or less) even with a serum bicarb of 45! Track the urine pH during potassium chloride supplementation and you’ll know they’re getting better (i.e. corrected chloride deficiency) when the urine pH suddenly jumps above 7 –(Metha, UpToDate 2021).
Acetazolamide
Acetazolamide induces a proximal renal tubular acidosis (Type II RTA) to slow bicarb reabsorption in the proximal tubule. Theoretically, metabolic alkalosis can depress respiratory drive to generate a compensatory respiratory acidosis. Thus, hypoventilation is a concern. In the DIABLO trial (Faisy, 2016), patients with COPD and mechanical ventilation were given acetazolamide to correct metabolic alkalosis in hopes of improving respiratory drive. They found a nonsignificant decrease in time spent on mechanical ventilation in the acetazolamide group (read NephJC discussion here).
Kashlak Pearl – Dr. Topf recommends giving acetazolamide 500 mg twice daily to help lower the bicarb (a usual response is a drop of about six points e.g. from 45 to 39). Monitor the urine pH, which should become elevated once acetazolamide starts working.
Spironolactone
Should potassium supplements, acetazolamide, and spironolactone be continued at hospital discharge? Dr. Topf notes that acetazolamide is intolerable as a long term therapy because it makes any carbonated beverages taste terrible (Muñoz, 2018). Potassium supplements might be continued at discharge, but lower doses will probably be sufficient once aggressive diuresis has ceased (expert opinion). The same goes for spironolactone as normal chronic doses are in the 25-50 mg range (UpToDate 2021) and these high doses can cause sexual side effects (gynecomastia, loss of libido, etc).
Milk Alkali Syndrome
It’s a bit unclear which comes first the acute kidney injury (AKI) or the hypercalcemic, metabolic alkalosis. Hypercalcemia decreases the GFR (Medarov, 2009). And with decreased GFR the kidneys are unable to clear the calcium and bicarb, and we are “off to the races”. Dr. Topf notes that classic milk alkali from milk consumption featured elevated phosphorus, but modern milk alkali syndrome typically has low phosphorus because calcium carbonate is a good phosphate binder.
Historical note: Ingestion of milk and sodium bicarbonate to treat peptic ulcer disease (PUD) was the classic cause of milk alkali syndrome. This went away with the advent of new therapies for PUD. Modern milk alkali is largely due to calcium carbonate supplements in patients looking to treat or prevent mineral bone diseases (Yu, UpToDate 2021).
Treat milk alkali by stopping supplements and giving normal saline (replaces chloride and corrects volume depletion) at a rate as fast as you can (Yu, UpToDate 2021).
Kashlak Pearl – Most AKIs have metabolic acidosis and hypocalcemia. Thus, think of milk alkali in patients who have a metabolic alkalosis with hypercalcemia. With significant hypercalcemia, make sure to rule out dangerous causes like cancers.
Excess Mineralocorticoid Activation
Hyperaldosteronism illness script: Hypertension, hypokalemia, metabolic alkalosis, and worsening of hypokalemia with diuretics. Look for a suppressed renin and elevated aldosterone, though a normal plasma aldosterone is not sensitive enough to rule out hyperaldosteronism (Hung, JCEM 2021).
Syndrome of apparent mineralocorticoid excess (SAME) is loss of function of 11-beta-hydroxysteroid dehydrogenase (He, 2020). How does it work? Cortisol has the capacity to activate mineralocorticoid receptors. It circulates at 100 times the concentration of aldosterone (Young, UpToDate 2021). The 11-beta-hydroxysteroid dehydrogenase enzyme is necessary to deactivate cortisol and prevent it from overpowering aldosterone as a signal at the mineralocorticoid receptors. Thus, patients with 11-beta-hydroxysteroid dehydrogenase deficiency have hypertension and hypokalemia and present just like hyperaldosteronism except aldosterone levels are suppressed. This enzyme is deactivated by glycyrrhetinic acid in black licorice (Touyz, 2008). Here’s the case report of a fatal dose of black licorice from NEJM.
Diagnose the Cause of Metabolic Alkalosis
How can we figure out the cause of metabolic alkalosis? Look at the urinary chloride.
Low urine chloride
Patients with low urine chloride, under 20 mEq/L (e.g. vomiting, milk alkali, volume depletion, diuretics) will respond to chloride replacement (e.g. potassium chloride supplements). Urine sodium as a measure of volume depletion is less reliable in patients with metabolic alkalosis because it is attracted to urinary bicarb and thus falsely elevated (Emmett, UpToDate 2021).
Elevated urine chloride
Metabolic alkalosis driven by mineralocorticoid receptor activation (hyperaldosteronism, SAME, Cushing’s syndrome) will have high urinary chloride, above 20.
Take Home Points
- Use normal saline NOT balanced solutions.
- Fix the potassium.
- Look at the urine chloride.
- These patients have increased mortality (Anderson, 1987). Be vigilant and treat associated electrolyte disturbances (e.g. Ca, K, etc.).
See prior Curbsiders episodes on Acid-Base and RTA with @Kidney_Boy
#104: Renal tubular acidosis with Kidney Boy, Joel Topf MD
#88: Acid base, boy bands, and grandfather clocks with Joel Topf MD