This blog and the posts on it are my study notes which I put up to help me reinforce my learning on the subjects I review.
I’m reviewing all of the excellent diagnostic schemas from the Clinical Problem Solvers.
And today I review the diagnostic schema Syncope [This link is to the web page where the video of the schema is discussed. Be sure to review the video].
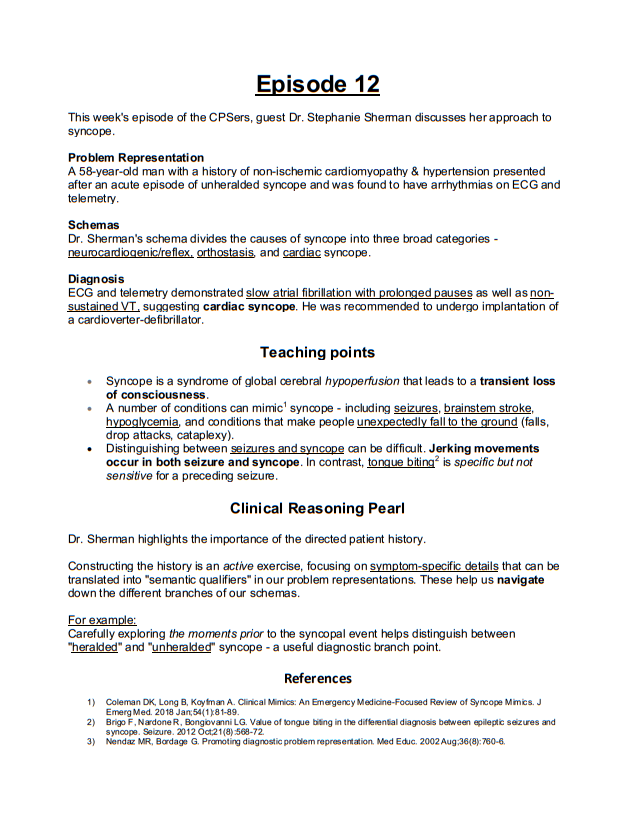
Dr. Sherman shares her Can’t Miss Diagnoses for Syncope
Cardiac syncope is a do not miss diagnosis that is often associated with high risk features on the patient’s history.
Ask about syncope with exertion.
Ask about lack of a prodrome so out of the blue that the patient may even sustain trauma without time or warning to protect yourself.
Ask about syncope while supine or syncope that occurs with an abnormal ECG or in a patient with a history of heart disease.
And here is more of Dr. Sherman’s discussion of the Syncope diagnostic schema:
I’m excited to share my diagnostic approach to syncope.
Defining syncope: a state a state of global hypo perfusion leading to transient loss of consciousness with spontaneous recovery.
Simply put syncope happens because the brain doesn’t get enough blood flow and thus the patient passes out.
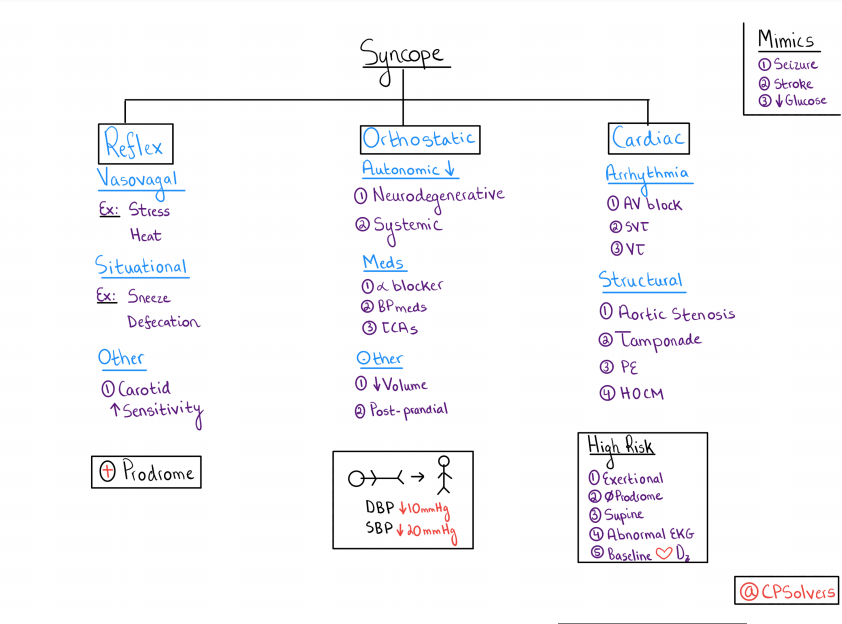
Syncope mimics are conditions that cause transient loss of consciousness for reasons other than low blood flow to the brain.
Seizure, stroke specifically in the brainstem which controls wakefulness, and hypoglycemia.
It is important to note that while we commonly associate seizure with involuntary muscle movement and loss of bladder control, syncope from any cause can also be associated with myoclonus jerking and with incontinence.
The three main categories of syncope are reflex, orthostatic, and cardiac.
Reflex syncope is also called neural cardiogenic syncope.
All categories of reflex syncope are associated with high vagal tone such as dizziness, nausea, or sweating before the patient passes out.
Orthostatic Syncope:
Measuring orthostatic of blood pressure is a critical component of syncope evaluation. To do so have the patient lie flat for five minutes and record the blood pressure.
Then, have the patient stand up, and at one and three minutes after standing before the blood pressure and ask about symptoms
Orthostatic vital signs are positive if the diastolic blood pressure drops by 10 or the systolic blood pressure drops by 20 in a symptomatic patient.
The third category of syncope is cardiac which includes arythmogenic causes, and structural causes.
Please note that several of these cardiac structural problems (aortic stenosis, pulmonary embolus, temp nine, and hypertrophic obstructive cardiomyopathy) can lead to orthostasis as well.
Here is the link to the Syncope podcast:
Here are the diagnostic schema for Syncope Version 1 [Link is to the PDF] and here is the diagnstic schema for Syncope Version 2 [Link is to the PDF] and after the diagnostic schemas below I have placed a copy of the show notes of Episode 12 [Link is to the PDF]:
Syncope Version 1
Syncope Version 2

Show Notes For Episode 12