
Lactate Measures: When, Why, and How Much, 1:02:23, 2013, YouTube video from Critical Care. [Please note these authors are discussing adult sepsis]
The speakers for this lecture are Drs. Tom Shaughnessy, and R. Phillip Dellinger. The moderator is Dr. Shawn Townsend.
1:21: Dr. Shaughnessy speaks first and all that follows until is Dr. Shaughnessy.
2:54: Lactate: A marker of malperfusion, not a pseudonym for sepsis.
- Other manifestations of end-organ dysfunction
- hypotension
- bilateral infiltrates
- coagulopathy, thrombocytopenia
- oliguria, elevated creatinine
- elevated bilirubin
- Lactic acidosis has multiple causes
- Most are type A–caused by hypoperfusion [the overwhelming majority of elevated lactate are type A, the speaker says, later in the talk]
- Type B: mitochondrial toxins, etoh, malignancy, metabolism errors
- Of available biomarkers, Lactate has the most support adverse outcomes.
4:04: Absence of an elevated lactate is not evidence absence of sepsis. 15 to 30% of septic patients will have other evidence of end-organ dysfunction despite a normal lactate.
4:36: [Thus] not every case of severe sepsis has an elevated lactate. But that in fact in no way diminishes the importance of lactate as a marker for sepsis.
5:27: And not all elevated lactate is due to sepsis–there are other causes–see Above type A and Type B.
6:34: Typically, when you have an elevated lactate, you have a patient to whom something bad is happening. It may or may not be sepsis but it is definitely worthy of further care.
7:29: Lactate best uses: Screening Tool
- Screening vs diagnosis
- Must assume sepsis [is the cause of the lactate elevation] until proven otherwise [since sepsis is by far the most common cause of elevated lactate]
- [Thus] it follows that appropriate treatment should follow until that time [that it is proved it is not sepsis]
10:37: Lactate best uses: As a monitor of clinical trajectory
- Trigger for EGDT (Early Goal Directed Therapy)
- Serial assessments to guide EGDT management
- a part of ongoing resuscitation management (getting worse or getting better)
10:54: When to Order Lactate?: Admission
Predictive value of admission lactate becomes significant at 2-2.5 mM
- To identify cases of severe sepsis.
- Identify potential cases Severe Sepsis
- As a tool for level of care decisions (ICU, stepdown, floor)
13:47: Lactate Measurement: Optimal Time Intervals for serial assessment:
- No definitive consensus
- Most studies use two to six hour intervals
Borderline patients (lactate 2 to 4 mmol)
- Next day testing probably not optimal!
14:26: When the lactate testing interval is being used to guide therapy, the interval is one to two hours. When used for prognostic intervals it [the interval] can be up to 24 hours.
16:01: Lactate site of assessment:
- Gold standard: arterial blood
- POC (point of care) testing has high accuracy vs. lab measurements.
- Venous and capillary results tend to overestimate vs. arterial but most studies find satisfactory agreement. (0.2 mM bias)
- Venous and capillary sources offer ease, speed, and consistency of testing. For screening purposes, this may be the better screening tool.
18:00 to 18:50: Dr. Shaughnessy closes his remarks: “Screening is screening and diagnosis is diagnosis. So the purpose of screening is to capture not only all the established easy cases of severe sepsis but also those that are possibly severe sepsis. If you are not doing that, then you don’t have a screening program, you have a diagnosis program. If you are going to have a screening program that works upfront–that triggers alerts and alarms–you are going to have to accept the fact that you are always going to have an N in your screening program that is much greater than the number of patients who ultimately get diagnosed.”
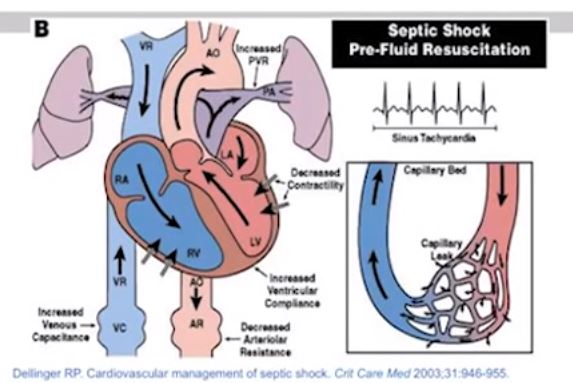
19:00 The next section is by Dr. Dellinger and is titled “Quantitative Protocolized Resuscitation of Sepsis Induced Tissue Hypoperfusion–Choosing the Target(s)
19:43: The slide below is a summary of all the things that happen in sepsis.
20:42: The speaker recommends that each hospital have their protocol for sepsis induced hypoperfusion that everyone in the institution signs in to. [There are examples of such protocols on Surviving Sepsis Campaign Protocols and Checklists.]
20:46: The Plan (of the Bundles or Protocols) is discussed.
21:46: Fluid Therapy:
Initial fluid challenge in sepsis induced in tissue hypoperfusion (hypotension or elevated lactate) with suspicion of hypovoleumia to be a minimum of 30 ml/kg of crystalloids (a portion of this may be albumin equivalent). More rapid administration and greater amounts of fluid, may be needed in some patients.
26:00: Here the speaker discusses some targets of therapy [Central Venous O2 pressure and central venous pressure] that may no longer be relevant (See Surviving Sepsis Campaign Statement Regarding Hemodynamic and Oximetric Monitoring in Response to ProCESS and ARISE Trials October 1, 2014)
26:10: Dr. Dellinger discusses lactate clearance and goes over the article, Lactate Clearance vs. Central Venous Oxygen Saturation as Goals of Early Sepsis Therapy, in JAMA in 2010 (see Resources). The study concluded that “Among patients with septic shock who were treated to normalize central venous and mean arterial pressure, additional management to normalize lactate clearance compared with management to normalize ScvO2 did not result in significantly different in-hospital mortality.”
28:10: [The above conclusion] has been used as an argument by some people that lactate clearance should be used as an alternative to targeting ScvO2 in patients with sepsis induced hypoperfusion. [This discussion may now be moot. See reference (3)]
28:25 to 30:16: He then goes on to discuss aspects of the study and article that still are instructive.
30:29: “With tissue hypoperfusion associated elevated lactate levels [we] suggest targeting lactate normalization as rapidly as possible” [rather than being satisfied with a 10-20% decline–If you went from 10 mMol to 8 mMol with resuscitation, should you be happy? the speaker asks. We felt good about getting rid of lactate but not about a 10% reduction]
34:10 to 1:02:23: Questions and panel discussion
35:25: The threshold for admission to the hospital is 2.0 to 2.5 mMol. And where in the hospital is determined by the other clinical details and by the available resources.
35:43: Dr. blank again highlights the difference between lactate as a screen and lactate as diagnostic tool and for following treatment.
37:02 to 38:02: Dr. Shaughnessy: “When we follow the trajectory of a resuscitation, we are looking for a resolution of that lactate and there is pretty strong evidence that when you use that threshold level trigger level of 2.0 or 2.5 that is where you start getting the significant mortality changes. So that is where you can, I guess, breath a little easier once they are resuscitated to that degree. The question is how often should look at that [meaning lactate level] since many here people are getting grief for how many lactates are being ordered. But it is a relatively convenient test and as a biomarker of resolution of malperfusion regardless of whether it is due to sepsis or not–I actually think it is may be better thought of as a resuscitation end-point as opposed to a sepsis endpoint. “
38:47: Dr. Dellinger: “For total normalization of lactate, I think most intensivists would say that is my goal in a patient that I admit to the ICU with severe sepsis and a high lactate.”
41:27: There is a brief discussion of the PROcESS trial hypothesis from the perspective of 2012 (before it reported its results).
Resources:
(1) Surviving Sepsis Campaign: International Guidelines for Management of Severe Sepsis
and Septic Shock: 2012 [Full Text PDF].
(2) The 2012 Surviving Sepsis Bundles can be accessed here.
(3) Surviving Sepsis Campaign Statement Regarding Hemodynamic and Oximetric Monitoring in Response to ProCESS and ARISE Trials October 1, 2014
(4) Lactate clearance vs central venous oxygen saturation as goals of early sepsis therapy: a randomized clinical trial [PubMed Abstract], [Full Text in PMC]. JAMA. 2010 Feb 24;303(8):739-46. doi: 10.1001/jama.2010.158.



