
What follows is from the 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease. [Full Text HTML] [Full Text PDF]. Circulation. 2012; 126: e354-e471.
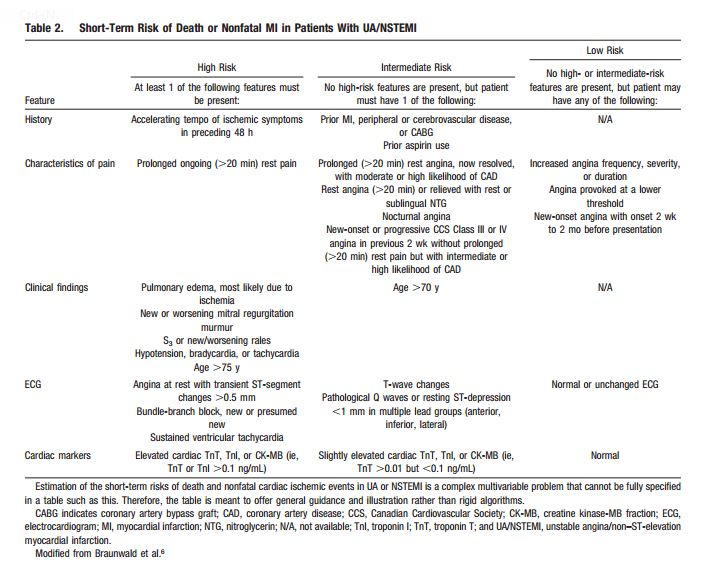
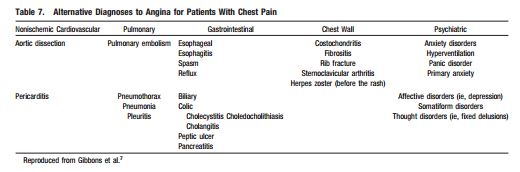
When a patient presents in any clinical encounter with the symptom of new or a change in established chest pain (by phone, in the office, urgent care center, or emergency department), the questions of Table 2 should be asked and answered first. In this way the patient with possible CAD symptoms can be classified into one of the three risk groups. Patients in the first two groups require immediate evaluation in the emergency department. Patients in the third group, can be evaluated using these 2012 ACCF/AHA guidelines. But after asking and answering the questions in Table 2, you also want to consider other possibly life threatening conditions presented in Table 7 which I have inserted right after table 2.
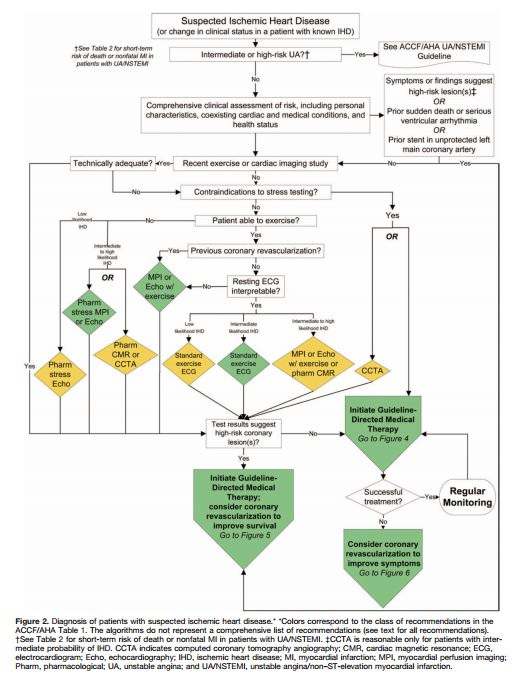
So you’ve reviewed Tables 2 and 7 and you decide that the patient can be evaluated in the office and that the initial diagnostic evaluation should be noninvasive. And so you proceed by using Flow Chart in Figure 2 below.
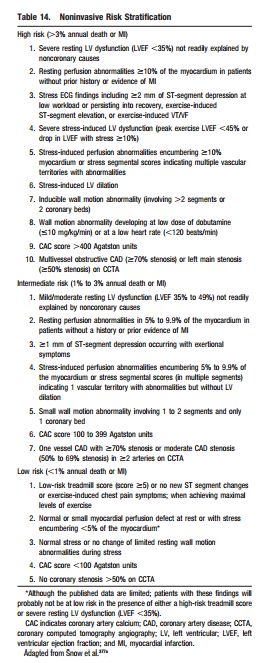
And then you look at the noninvasive workup to determine the risk of heart attack or death. If there are any high risk findings that suggest that revascularization might reduce his/her risk of death or serious heart damage, then you want to consider coronary angiography. Review w/u looking for the findings in Table 14. If the patient falls into high or intermediate risk, then serious consideration of coronary angiography is indicated to determine if revascularization can lessen that risk.
________________________________________________________________
What follows is a direct quote from the 2012 ACCF/AHA SIHD Guideline
3.3. Coronary Angiography
3.3.1. Coronary Angiography as an Initial Testing Strategy to Assess Risk: Recommendations
Class I
Patients with SIHD who have survived sudden cardiac death or potentially life-threatening ventricular arrhythmia should undergo coronary angiography to assess cardiac risk.349–351 (Level of Evidence: B)
Patients with SIHD who develop symptoms and signs of heart failure should be evaluated to determine whether coronary angiography should be performed for risk assessment.352–355 (Level of Evidence: B)
3.3.2. Coronary Angiography to Assess Risk After Initial Workup With Noninvasive Testing: Recommendations
Class I
Coronary arteriography is recommended for patients with SIHD whose clinical characteristics and results of noninvasive testing indicate a high likelihood of severe IHD and when the benefits are deemed to exceed risk.59,126,260,310,356–362 (Level of Evidence: C)
Class IIa
Coronary angiography is reasonable to further assess risk in patients with SIHD who have depressed LV function (EF <50%) and moderate risk criteria on noninvasive testing with demonstrable ischemia.363–365 (Level of Evidence: C)
Coronary angiography is reasonable to further assess risk in patients with SIHD and inconclusive prognostic information after noninvasive testing or in patients for whom noninvasive testing is contraindicated or inadequate. (Level of Evidence: C)
Coronary angiography for risk assessment is reasonable for patients with SIHD who have unsatisfactory quality of life due to angina, have preserved LV function (EF >50%), and have intermediate risk criteria on noninvasive testing.306,366 (Level of Evidence: C) ________________________________________________________________
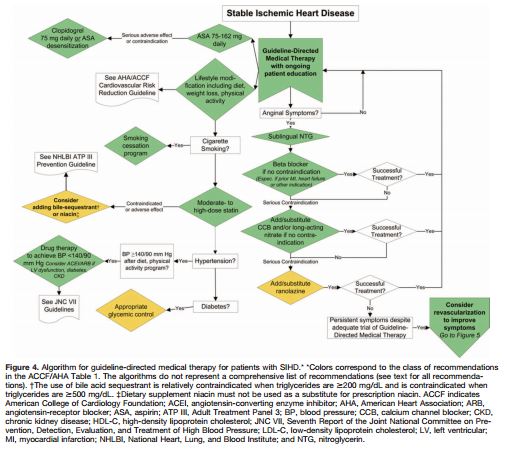
And the diagnosis of stable ischemic heart disease requires the initiation of guideline directed medical therapy as per Figure 4.
Resources:
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the Diagnosis and Management of Patients With Stable Ischemic Heart Disease. [Full Text HTML] [Full Text PDF].
An externally validated model for predicting long-term survival after exercise treadmill testing in patients with suspected coronary artery disease and a normal electrocardiogram. Ann Intern Med. 2007 Dec 18;147(12):821-8. [PubMed]



