
The following are excerpts from Reference (1), 2015 CUA Practice guidelines for erectile dysfunction [There are additional references in Resources at the end of this article]:
Questionnaires
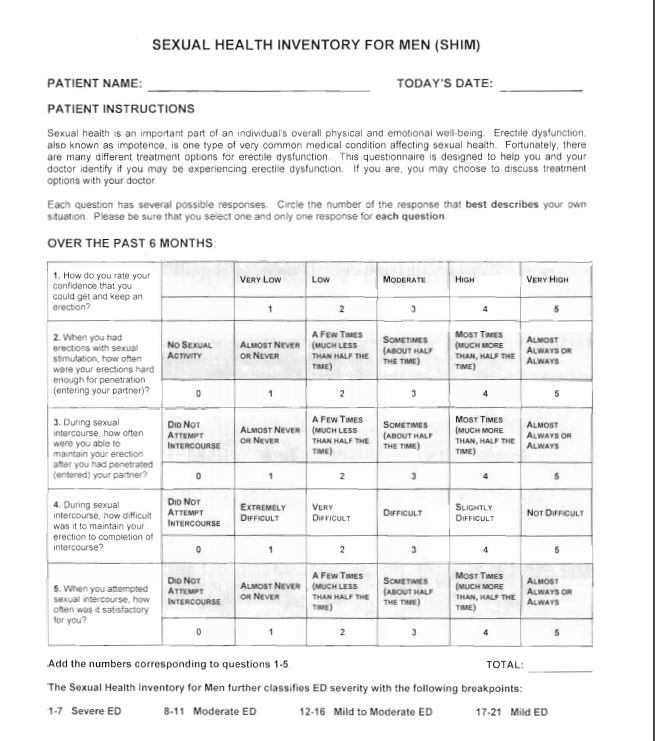
Use of validated questionnaires may be beneficial. These tools can be patient self-administered and provide much of the above information in an efficient non-threatening manner, while being time-saving and cost-effective.6 There are validated instruments designed to evaluate sexual and erectile function. The greatest utility of these questionnaires may be in establishing a response to therapy and determining overall satisfaction with drug use over a specified length of time (i.e., 4 weeks). The most common questionnaire is the SHIM [Here is a link to the PDF of the SHIM]:
Physical exam
The aim of a focused physical examination in men with ED is to examine genital anatomy and identify any related abnormalities (e.g., Peyronie’s plaques), endocrine signs, and possible comorbidities (neurological, vascular, and possible life-threatening conditions).10 An association exists between erectile dysfunction and peripheral vascular disease, as well as ED and the potential development of coronary artery disease.11Assessment should include body habitus (secondary sexual characteristics), peripheral circulation (ED is a predictor of cardiovascular morbidity and mortality, findings consistent when controlled for confounders), neurological and genitourinary systems.10 Testicular examination is important to ensure testes/testis presence and to examine consistency of the testicle (i.e., atrophy, hypogonadism). The identification of penile deformities may be best achieved in the erect state, but is most commonly examined by stretching the penis to make the Peyronie’s plaque(s) more pronounced. The physical examination can also be a source of embarrassment or discomfort for some patients; therefore, every effort should be made to ensure privacy and personal comfort.
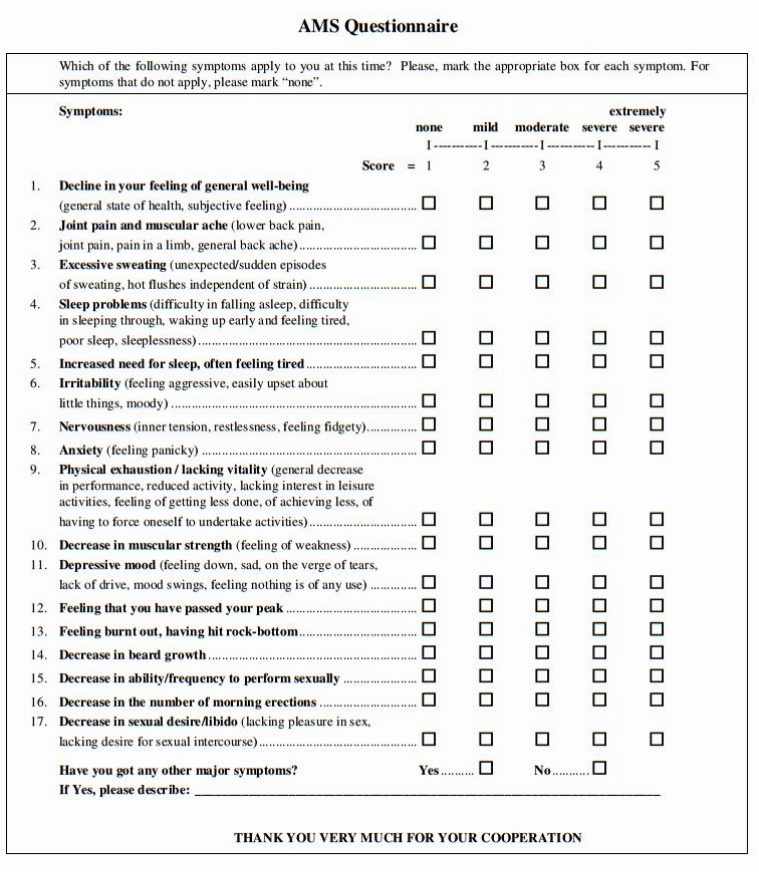
Erectile dysfunction can be caused or made worse by a number of serious medical problems including put in list from Ref (3) to be determined.
I use the Aging Male Symptom Scale (AMS) [link is to the PDF] which of the above may be causing or aggravating the erectile dysfunction:
Laboratory testing
Overview
The recommendations by the International Society for Sexual Medicine’s International Consultation on Sexual Medicine suggest that laboratory tests for men with sexual problems may include fasting glucose, lipid profile and, in select cases, a hormone profile. Hormone profiles are used to identify or confirm specific etiologies (e.g., hypogonadism) or to assess the role of potential medical comorbidities or concomitant illnesses.6,12
Assessment for occult diabetes may be performed with a fasting glucose or HbA1c. Although recommended by the WHO consensus panel, the lipid screen is considered an optional component of the Canadian ED assessment but is suggested as a valuable addition to the evaluation and good general practice.2
Hormonal profile screening remains a controversial aspect of the routine evaluation of ED. There is a general guideline agreement that in a man with ED and hypoactive desire, incomplete response to PDE5-inhibitor treatment, and in all men with known diabetes (as suggested by 2013 Canadian Diabetes Association guidelines)2 testing and potential treatment for low levels of testosterone is appropriate. In men with normal desire and ED the need for global testing is controversial and currently undetermined. In the appropriate patient, once treatment with exogenous testosterone is initiated, ongoing follow-up is mandatory according to published guidelines.12,13
For men with diabetes, the 2013 Canadian Diabetes Association guidelines also support annual review of sexual function and determination of testosterone levels.
Optional testing such as thyroid-stimulating hormone (TSH), luteinizing hormone (LH) and follicle-stimulating hormone (FSH), prolactin, complete blood count (CBC), and urinalysis are considered complementary and not felt to be mandatory in the evaluation of ED in most cases, but are added when dictated by clinical context.3,6,10
There are a number of specialized tests that are discussed in the paper. These include:
- Psychological or Psychiatric Assessment
- Nocturnal penile tumescence and rigidity testing (NPTR)
- Vascular Testing
- Endocrinologic Tests Resource (4)
- Neuro-psychological testing
Resources:
(1) 2015 CUA Practice guidelines for erectile dysfunction [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Can Urol Assoc J. 2015 Jan-Feb; 9(1-2): 23–29.
doi: 10.5489/cuaj.2699
(2) A critical analysis of the 2014 CUA guidelines for erectile dysfunction: Is there more that can be done? [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Can Urol Assoc J. 2015 Jan-Feb;9(1-2):30-1. doi: 10.5489/cuaj.2731.
(3) Nocturnal penile erections: the role of RigiScan in the diagnosis of vascular erectile dysfunction. [PubMed] [Ref list]. Elhanbly S, Elkholy A. J Sex Med. 2012 Dec; 9(12):3219-26.
(4) “Diagnosis, Management and Treatment Of Testosterone Deficiency” From The Canadian Urological Association Posted on November 17, 2016 by Tom Wade MD
(5) The Management of Erectile Dysfunction: An Update June 2007 From The American Urologic Association [Full Text PDF]



