
This post is Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 3 Of 4 – 2 to 24 Months – Pneumonia from the outstanding Approach To Febrile Infants In The Emergency Department lecture and accompanying slides from The Children’s Hospital of Philadelphia (CHOP).
I’ve divided the above CHOP lecture into four posts:
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 1 Of 4 – Less Than 60 Days Of Age
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 2 Of 4 – 2 to 24 Months – Occult Bacterial Infections – UTI
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 3 Of 4 – 2 to 24 Months – Pneumonia
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 4 Of 4 – 2 to 24 Months – Occult Bacteremia
Here are links to the three clinical pathways from CHOP that are relevant to the lecture:
- ED Pathway for Evaluation/Treatment of Febrile Young Infants (0-56 Days Old)
- Pathway for Evaluation/Treatment of Child with Fever
- Pathway for Evaluation And Treatment Of Child With Community-Acquired Pneumonia
Here is the link to The Clinical Pathways Library [a comprehensive list of the clinical pathways at Children’s Hospital of Philadelphia (CHOP)].
For a complete list of the outstanding pediatric FOAM courses from the Children’s Hospital of Philadelphia, please see CHOP Open-access Medical Education.
So here are some of the slides and lecture notes from Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 3 Of 4 – 2 to 24 Months – Pneumonia.
Slide 1:
Slide 2:
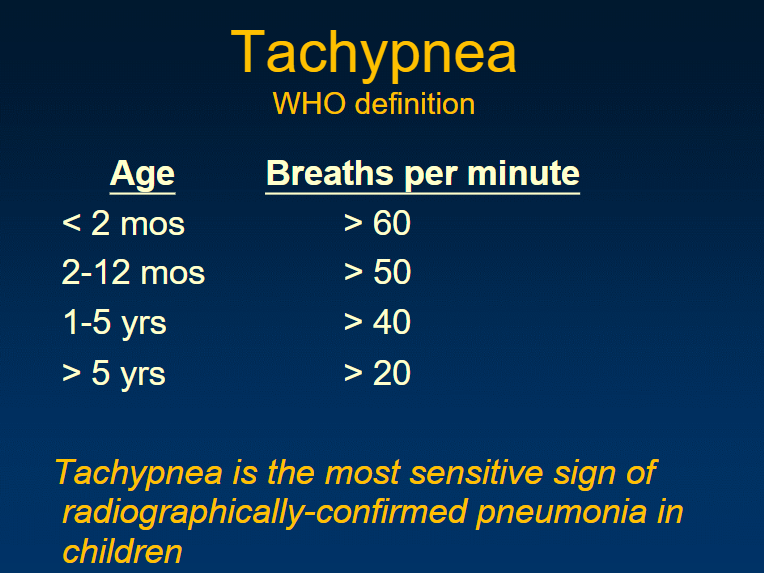
Slide 33:
So probably the best clinical finding for pneumonia we have is the respiratory rate or tachypnea.
I have the mother undress the baby and I watch and I see what the respiratory rate is and if there is work of breathing. If the respiratory rate is totally normal and there is no work of breathing, even if they are crying and screaming, I feel much more reassured than trying to get an exam on a crying baby.
So again, tachypnea, work of breathing assessment from across the room may better than your stethoscope in that nine months to two years of age group.
Slide 34:
Slide 35:
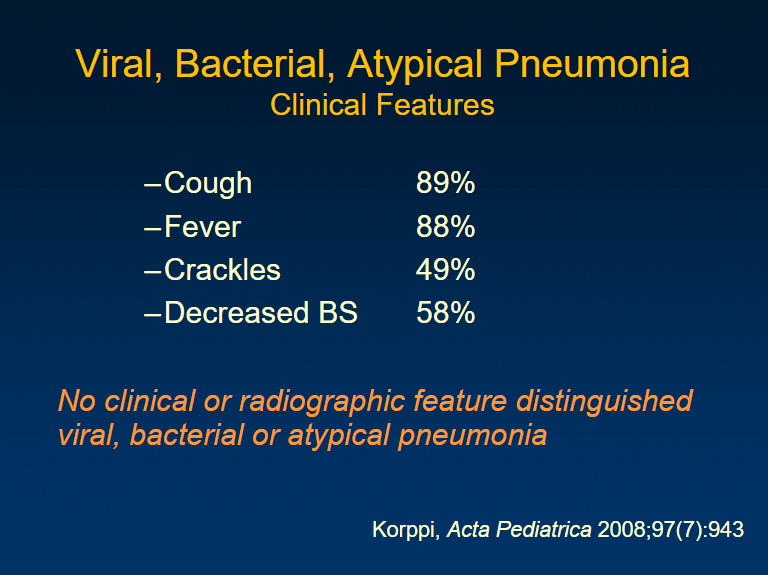
Pneumonia, when do you think about it? It often follows a viral respiratory infection. So that case of where they’ve had a cold. You’d expect the cold to be going away and all of a sudden they have a fever and worsening cough.
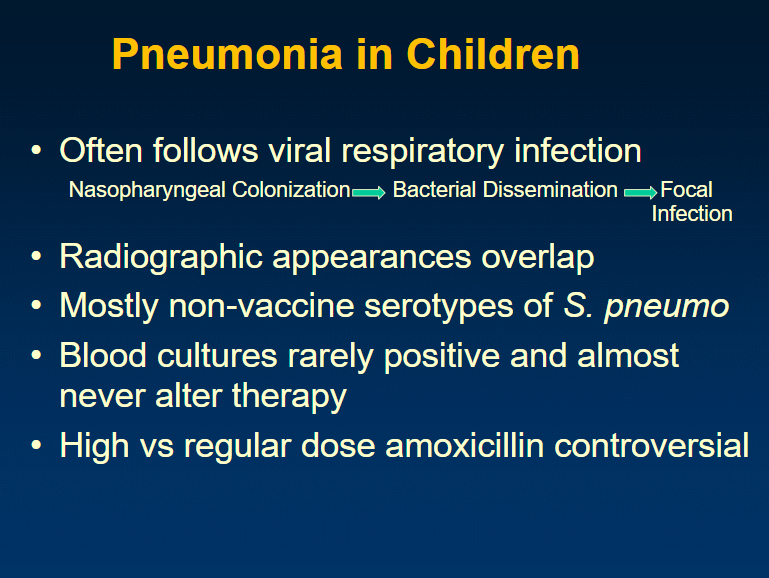
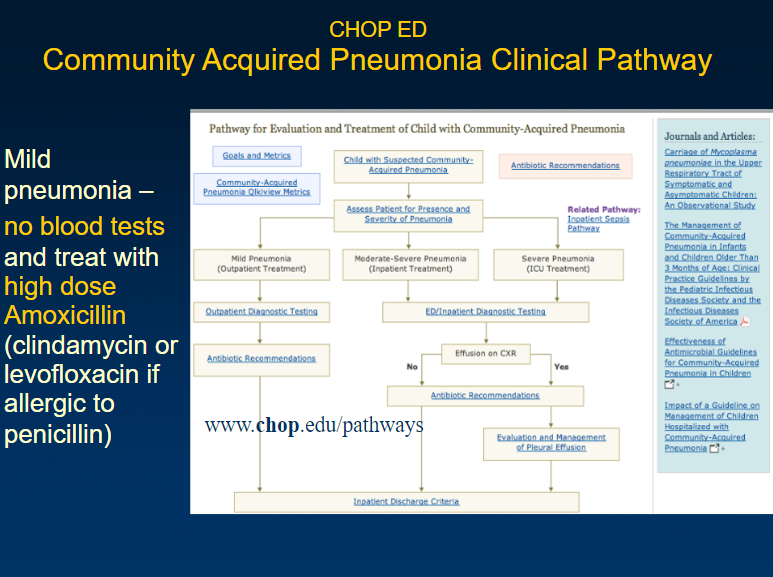
Slide 36:
Pathway for Evaluation And Treatment Of Child With Community-Acquired Pneumonia
Here is the above CHOP lecture into my four four posts:
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 1 Of 4 – Less Than 60 Days Of Age
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 2 Of 4 – 2 to 24 Months – Occult Bacterial Infections – UTI
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 3 Of 4 – 2 to 24 Months – Pneumonia
- Evaluation Of The Well Appearing Febrile Infant From CHOP – Part 4 Of 4 – 2 to 24 Months – Occult Bacteremia
Here are links to the three clinical pathways from CHOP that are relevant to the lecture:
- ED Pathway for Evaluation/Treatment of Febrile Young Infants (0-56 Days Old)
- Pathway for Evaluation/Treatment of Child with Fever
- Pathway for Evaluation And Treatment Of Child With Community-Acquired Pneumonia
Resources:
(1) NICE Guideline – Fever in under 5s: assessment and initial management
Clinical guideline [CG160] Published date: May 2013 Last updated: August 2017
(2) Validation of the “Step-by-Step” Approach in the Management of Young Febrile Infants [PubMed Abstract] [Full Text HTML] [Download Full Text PDF]. Pediatrics. 2016 Aug;138(2). pii: e20154381. doi: 10.1542/peds.2015-4381. Epub 2016 Jul 5.
The above article has been cited by 12 articles in PubMed Central.
(3) Thermometry in paediatric practice [PubMed Abstract] [Full Text] [Full Text PDF]. Arch Dis Child. 2006 Apr;91(4):351-6
(4) Reaffirmation of AAP Clinical Practice Guideline: The Diagnosis and Management of the Initial Urinary Tract Infection in Febrile Infants and Young Children 2–24 Months of Age [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Pediatrics. 2016 Dec;138(6). pii: e20163026.
The above article has been cited by 7 PubMed Central articles.
(5) Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Pediatrics. 2011 Sep;128(3):595-610. doi: 10.1542/peds.2011-1330. Epub 2011 Aug 28.
(6) Urinary Catheterization in Infants: When It’s Knot so Simple [PubMed Abstract] [Full Text]. Clin Pract Cases Emerg Med. 2018 Jan 11;2(1):55-57. doi: 10.5811/cpcem.2017.11.36438. eCollection 2018 Feb.
(7) PURLs: An easy approach to obtaining clean-catch urine from infants [PubMed Abstract] [Full Text] [Full Text PDF]. J Fam Pract. 2018 Mar;67(3):166-169.
(8) NW Newborn Clinical Guideline – Urinary Catheterisation Accessed 12-18-2018.
(9) Catheterization of the Urethra in Male Children YouTube video from the New England Journal Of Medicine.



