Today, I review, link to, and excerpt from The characterisation of subjective cognitive decline from Lancet Neurology [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Lancet Neurol. 2020 Mar;19(3):271-278. doi: 10.1016/S1474-4422(19)30368-0. Epub 2020 Jan 17.
There are 135 similar articles in PubMed.
The above article has been cited by 446 articles in PubMed.
All that follows is from the above article.
Discrimination of SCD from MCI
The absence of objective cognitive impairment distinguishes SCD from MCI. In principle, MCI was developed as a diagnostic entity, whereby the absence or presence of cognitive impairment is decided on the basis of clinical judgment. Cognitive test performance of the patient can support this diagnostic judgement.3 When clinical judgement is used alone, there may be a diagnostic overlap of SCD and MCI between clinicians However, in many clinical settings, the distinction between SCD and MCI is mainly based on either short or extended psychometric tests.3,15 When differentiating MCI (impaired objective performance) from SCD (unimpaired objective performance) on the basis of psychometric tests, we consider short cognitive screening tests, such as the Mini-Mental State Examination or the Montreal Cognitive Assessment, to have limited diagnostic accuracy.16 Instead, we suggest comprehensive neuropsychological test batteries that assess multiple cognitive domains, and for which age-adjusted, sex-adjusted, and education-adjusted normative data are available.17
Abstract
A growing awareness about brain health and Alzheimer’s disease in the general population is leading to an increasing number of cognitively unimpaired individuals, who are concerned that they have reduced cognitive function, to approach the medical system for help. The term subjective cognitive decline (SCD) was conceived in 2014 to describe this condition. Epidemiological data provide evidence that the risk for mild cognitive impairment and dementia is increased in individuals with SCD. However, the majority of individuals with SCD will not show progressive cognitive decline. An individually tailored diagnostic process might be reasonable to identify or exclude underlying medical conditions in an individual with SCD who actively seeks medical help. An increasing number of studies are investigating the link between SCD and the very early stages of Alzheimer’s disease and other neurodegenerative diseases.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Introduction
With an ageing population, concerns about cognitive decline are becoming an increasingly relevant topic that arises during medical consultations. Concerns about cognitive decline can be associated with different objective levels of cognitive and functional impairment, which are revealed by clinical and neuropsychological examinations. Dementia is the most severe level of impairment and is defined by cognitive deficits that impair daily functioning and lead to loss of independence.1,2 Similar to dementia, mild cognitive impairment (MCI) is also characterised by objective cognitive impairment. However, by contrast with dementia, the day-to-day functioning of individuals with MCI remains largely intact and independence is preserved.3 Some individuals experience a subjective decrease in cognitive function, but cognitive performance by neuropsychological testing and in daily functioning shows no evidence of objective cognitive impairment. In clinical practice, these individuals are generally considered healthy. Regardless of the absence of evidence for objective cognitive impairment, the subjective decline in cognitive function experienced by individuals might become increasingly important for clinicians, because the number of individuals with such concerns who seek medical help and advice is growing. In 2014, the term subjective cognitive decline (SCD) was conceived by researchers to describe this condition, which has received increasing attention because of evidence of its association with an increased risk of future objective cognitive decline.4–6
One aim of this Personal View is to propose diagnostic and counselling considerations to health-care providers for individuals who seek medical help for SCD. Importantly, we do not propose actively searching or screening for individuals with SCD within or outside the clinical setting. A second aim is to provide information about the research findings and priorities for SCD to date, with a particular focus on studies looking at associations between SCD and preclinical Alzheimer’s disease within current research frameworks.
Definition and characterisation of SCD
The association between subjective decline in cognitive functioning and ageing, objective performance, and the future risk of cognitive decline has been addressed in diverse concepts and in various studies since the 1980s.7 In 2014, an international working group of researchers and clinicians, known as the SCD-initiative (SCD-I), proposed a common framework for SCD research that provided standardised terminology and criteria.4 The proposed SCD criteria were developed within the context of Alzheimer’s disease research; however, we believe that the same SCD criteria can also be useful in the health-care setting. The SCD criteria include two major features. First, a self-experienced persistent decline in cognitive capacity, compared with a previously normal cognitive status, which is unrelated to an acute event. This criterion infers that SCD reflects a state of cognitive decline from the perspective of the individual; observation of such a decline by others is not required. The second criterion is normal performance on standardised cognitive tests used to classify MCI, adjusted for age, sex, and education. As such, the individual’s cognition is unimpaired from an objective standpoint. Conditions that are defined by objective cognitive impairment, such as MCI or dementia, are distinct from SCD. Of note, SCD is not a diagnostic category of the International Statistical Classification of Diseases-10, the International Classification of Diseases-11, and the Diagnostic and Statistical Manual of Mental Disorders-5.
SCD is a broad condition that develops differently over time as a result of the variety of potential underlying causes (figure 1). To identify the potential causes of SCD in an individual, we propose that the concern of cognitive decline is evaluated by obtaining the following information from them: (1) which cognitive domains are affected (eg, memory, language, executive functioning, visual–spatial abilities, orientation, and attention); (2) whether specific worries are associated with the cognitive decline; (3) when the onset of cognitive decline occurred; (4) whether there is an association with any physical or mental conditions; and (5) whether there is an association with the use of medication, alcohol, or other substances.
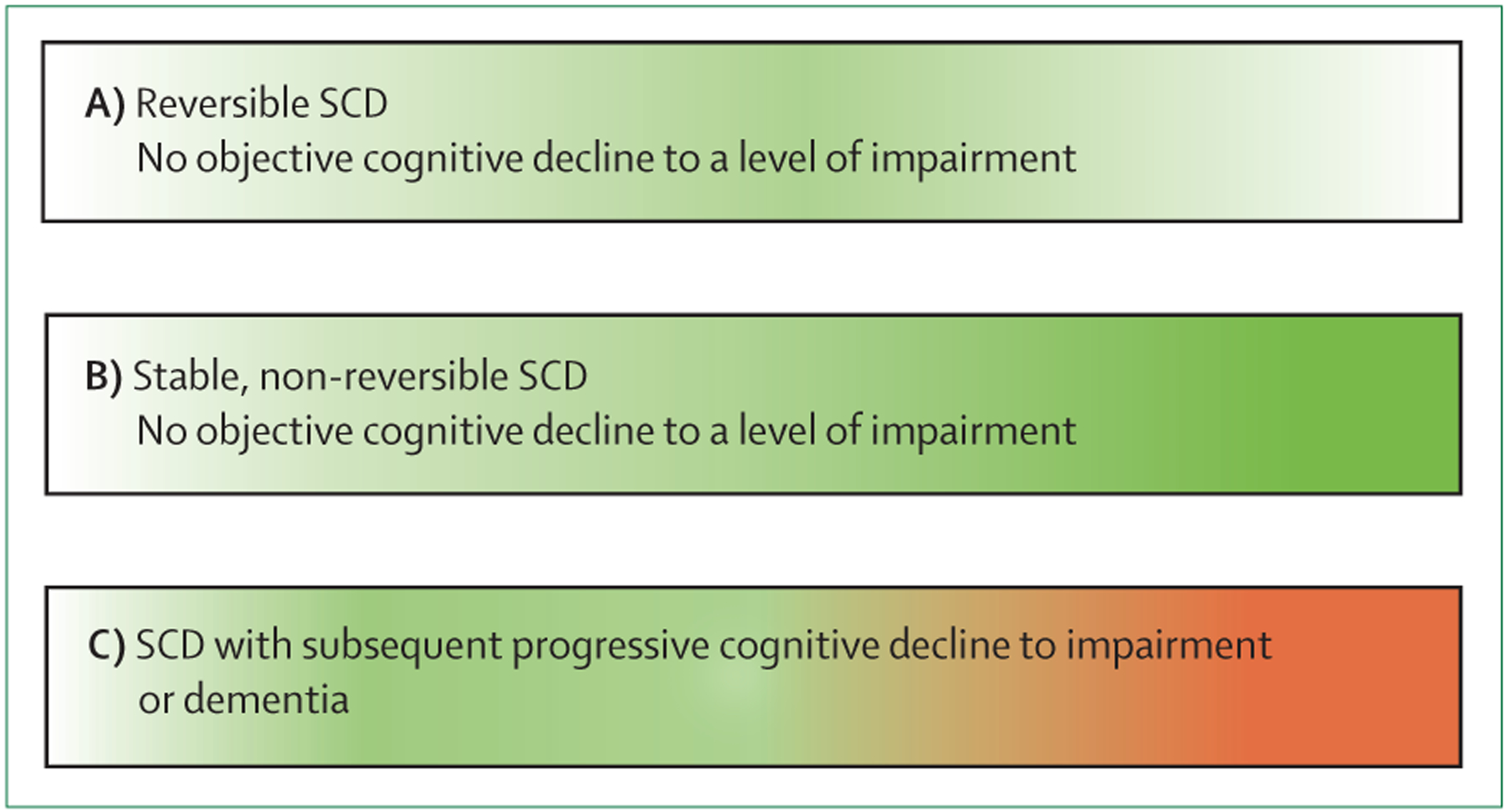
Figure 1: Schematic representation of trajectories of SCD and objective cognitive function over time.
(A) SCD occurs but remits fully, and objective cognitive functions remain stable. Conditions underlying SCD include depression, side-effects from medication, or intermittent sleep disturbances. (B) SCD occurs and continues without remitting (continuous green colour); objective cognitive functions remain largely stable. The normal ageing process can be an underlying cause of this type of SCD. (C) SCD occurs and objective cognitive functions subsequently deteriorates to dementia. This deterioration can be caused by neurodegenerative disease, including, but not limited to, Alzheimer’s disease. The proportion of individuals in each of the three SCD trajectories has not yet been fully delineated; however, the majority of individuals with SCD will not decline to dementia. The colour scheme indicates an absence of SCD (white), SCD (green), and objective impairment or dementia (red). SCD=subjective cognitive decline.
To characterise the concern of cognitive decline further, particularly with regards to severity, several additional tools are available.8 Examples include the Cognitive Function Index,9 the Cognitive Change Index,10 the Everyday Cognition questionnaire,11 the Subjective Cognitive Decline questionnaire,12 the SCD interview,13 or a simple two-question approach about their decline in memory and any associated concerns.14 No single gold standard instrument or sufficiently validated cutoff on any scale can differentiate individuals with SCD from those without SCD in the clinical setting, where SCD is currently defined by use of the two basic SCD-I criteria.4 A validated cutoff would be useful for classifying specific groups of individuals and for quantifying the severity of SCD in a research setting. As such, research priorities of the SCD-I are to harmonise existing measures and create a validated SCD scale.8
Discrimination of SCD from MCI
The absence of objective cognitive impairment distinguishes SCD from MCI. In principle, MCI was developed as a diagnostic entity, whereby the absence or presence of cognitive impairment is decided on the basis of clinical judgment. Cognitive test performance of the patient can support this diagnostic judgement.3 When clinical judgement is used alone, there may be a diagnostic overlap of SCD and MCI between clinicians However, in many clinical settings, the distinction between SCD and MCI is mainly based on either short or extended psychometric tests.3,15 When differentiating MCI (impaired objective performance) from SCD (unimpaired objective performance) on the basis of psychometric tests, we consider short cognitive screening tests, such as the Mini-Mental State Examination or the Montreal Cognitive Assessment, to have limited diagnostic accuracy.16 Instead, we suggest comprehensive neuropsychological test batteries that assess multiple cognitive domains, and for which age-adjusted, sex-adjusted, and education-adjusted normative data are available.17 No universally accepted single cutoff exists to define cognitive impairment for the purpose of differentiating between SCD and MCI. Commonly proposed approaches, however, include standard deviation (SD)-based cutoffs (ie, scores of >1·5 SD below the normative mean on any test within a specific cognitive domain; scores of >1·0 SD below the normative mean on at least two separate tests of one cognitive domain; or a score of >1·0 SD below the normative mean in at least three cognitive domains).18 To differentiate between SCD and MCI, individuals with SCD would need to score higher than the cutoffs, whereas individuals with MCI or dementia would need to score below the cutoffs. Alternatively, a clinical decision that is based on all the available clinical and neuropsychological information might be used to determine the extent of cognitive impairment.19,20
Of particular note, individuals with SCD and cognitively unimpaired individuals without SCD are only distinguished by reported feelings of subjective cognitive decline, which are experienced by individuals with SCD and not in individuals without SCD. The distinction is not made by cognitive testing, because individuals with SCD and cognitively unimpaired individuals without SCD are, by definition, objectively unimpaired, and they both perform above the cutoff for impairment in cognitive tests.
Prevalence of SCD in an aging population
Multiple physiological and subthreshold disease-related mechanisms contribute to the decline in cognitive function with aging. Typically, such declines in cognitive function involve the cognitive domains of processing speed, executive functions, memory, and visuospatial abilities.21,22 Most individuals notice some cognitive changes with increasing age. Population-based studies14,23 suggest that between 50% and 80% of older individuals (aged 70 years and older) who perform within normal ranges on cognitive tests, report some form of perceived decline in cognitive functioning when asked.
SCD and risk of cognitive decline
A meta-analysis5 of longitudinal epidemiological studies of cognitively unimpaired individuals with SCD (with at least 4 years of follow-up data) found a future decline to dementia in 14% of individuals and a future decline to MCI in 27% of individuals. These estimates are limited by the inclusion of all age groups in the analysis.5 Despite this limitation and even though SCD is not related to progressive cognitive deterioration in most individuals, SCD could be an early indicator of future cognitive decline for some individuals.6 Long-term prospective studies24,25 in individuals who eventually went on to develop dementia, suggest that SCD occurs, on average, around 10 years before the dementia diagnosis.
Conclusions and future directions
Clinicians are faced with an increasing number of individuals who seek medical help because they experience a subjective decline in cognitive function. There is evidence that individuals with SCD are at a greater risk of future cognitive decline and dementia than individuals who are cognitively unimpaired and do not have subjective cognitive decline. SCD could also be the first symptom of incipient neurodegenerative disease. However, several medical conditions can cause SCD, and research suggests that SCD is not an indicator of future cognitive decline for most individuals. We propose that clinical decisions for individuals who actively seek medical help should be tailored according to their indidivual needs. We also propose that advice about maintenance of brain health should be given to individuals with SCD. There is a strong interest in exploring the potential role of SCD as an early sign of neurodegenerative disorders. This research might become relevant if SCD could be combined with biomarker-based neurodegenerative disease detection and early interventions in the future.
Panel: Features that increase the risk of cognitive decline (SCD plus).
Subjective decline in memory irrespective of function in other cognitive domains5,14
Onset of SCD at 60 years and older4
*Not part of the original SCD plus features.4 SCD=subjective cognitive decline.