
In this post I link to and excerpt from 5 Pearls on Treatment of Alcohol Use Disorder
Posted: November 7, 2018. By: Dr. Katharine Lawrence, Dr. Martin Fried, Dr. Irene Swanenberg and Dr. Shreya P. Trivedi of CoreIM.
Here are excerpts from the above:

The Above Graphic: Dr. Caroline Srisarajivakul-Klein for CoreIM
Pearl 1 (Throwback)
- Unhealthy alcohol use is a catch-all term meant to describe a spectrum of drinking ranging from risky use to alcohol use disorder. Alcohol use disorder (AUD) is a problematic pattern of alcohol use leading to clinically significant impairment or distress.
- Risky drinking is thought of as daily and weekly alcohol limits:
- For men less than 65 years: more than 4 drinks/day or 14 drinks/week for
- For women and men over 65 years: more than 3 drinks/day or 7 drinks/week
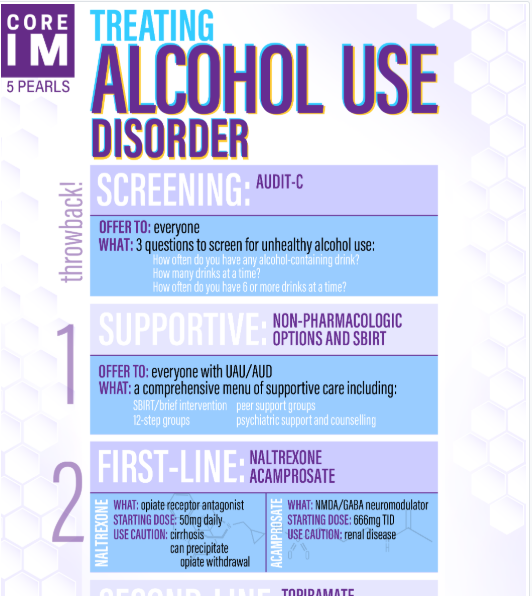
- The AUDIT-C tool* is the recommended screening tool for unhealthy alcohol use.
- A single-item screening question has also been validated: how many times in the last year, have you had more than three drinks (four drinks for men) in a day?
*Link is to the AUDIT-C tool on MDCalc.
Pearl 2
- First-line non-pharmacotherapies for AUD are captured in the mnemonic S-BIRT: screening, brief intervention, referral to treatment. It is a comprehensive approach identify and intervene in patient with unhealthy alcohol use. Basic tenets of BI include:
- raising the subject
- giving feedback about the level of risk
- encouraging the patient’s motivation to change, and
- setting goals or making a plan to implement that change.
- BI alone has not been shown to be effective in patients with alcohol use disorder
Pearl 3
- Patients who meet criteria for AUD should be offered medications in addition to non-pharmacologic therapies for treatment
- First-line pharmacotherapies for moderate to severe AUD include naltrexone and acamprosate
- Common side effects for naltrexone are largely gastrointestinal, and include abdominal pain, nausea, and diarrhea; naltrexone is contraindicated in patients with cirrhosis or who are actively using or at high risk for using opiates
- Acamprosate requires three-times-a-day dosing, and is not for use in patients with ESRD or CrCl<30; neuro-pysch side effects in including suicidality may also limit its use
Pearl 4
- Second-line pharmacotherapies include topiramate and gabapentin
- Their well-known side effect profiles (including memory impairment and somnolence, respectively) at the doses required to achieve efficacy may hinder their broader use in the outpatient setting
Pearl 5
- Novel therapeutic options currently under investigation for AUD include neuromodulation, nalmafene, and psychaedelics
- Neuromodulation, such as deep brain stimulation, is thought to work on the nucleus accumbens to target centers of reward behavior and reduce cravings
- Nalmafene is a long-acting k-opioid antagonist which is used in Europe
- Psychedelics like psilocybin and LSD are experiencing a resurgence in the study of a variety of diseases, including AUD, PTSD, and depression
See the Transcript that follows the 5 Pearls list in the show notes for additional details on the 5 Pearls.



