
In this post I link to and excerpt from Clinical Management of Stable Coronary Artery Disease in Patients With Type 2 Diabetes Mellitus: A Scientific Statement From the American Heart Association [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Circulation. 2020 May 12;141(19):e779-e806. doi: 10.1161/CIR.0000000000000766. Epub 2020 Apr 13.
All that follows are excerpts from the above article.
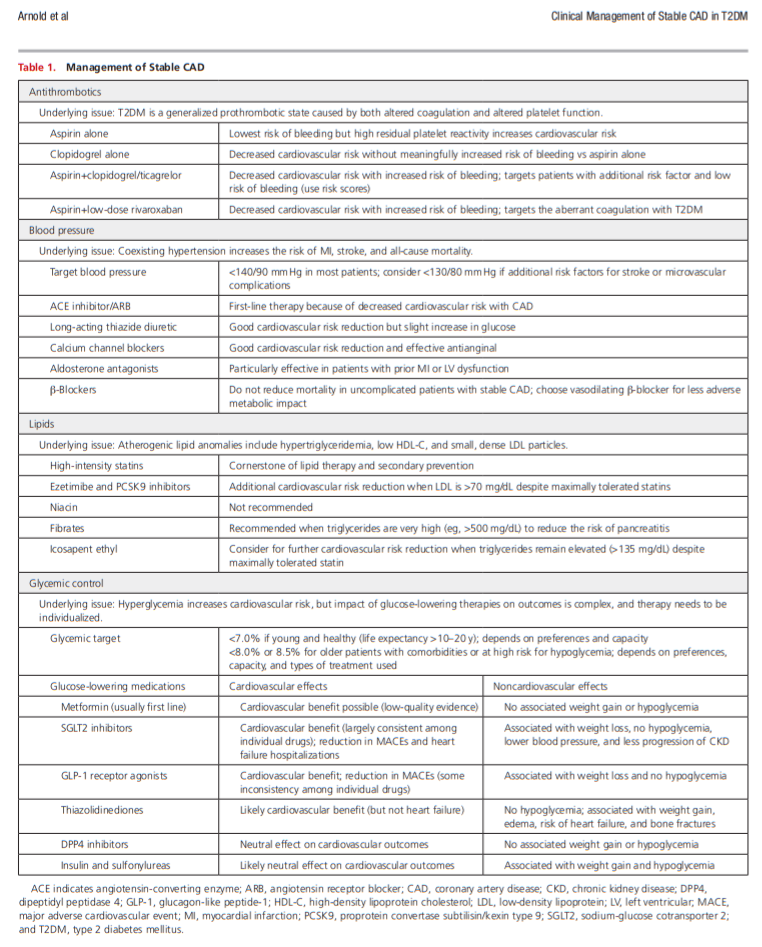
ABSTRACT: Although cardiologists have long treated patients with coronary artery disease (CAD) and concomitant type 2 diabetes mellitus (T2DM), T2DM has traditionally been considered just a comorbidity that affected the development and progression of the disease. Over the past decade, a number of factors have shifted that have forced the cardiology community to reconsider the role of T2DM in CAD. First, in addition to being associated with increased cardiovascular risk, T2DM has the potential to affect a number of treatment choices for CAD. In this document, we discuss the role that T2DM has in the selection of testing for CAD, in medical management (both secondary prevention strategies and treatment of stable angina), and in the selection of revascularization strategy. Second, although glycemic control has been recommended as a part of comprehensive risk factor management in patients with CAD, there is mounting evidence that the mechanism by which glucose is managed can have a substantial impact on cardiovascular outcomes. In this document, we discuss the role of glycemic management (both in intensity of control and choice of medications) in cardiovascular outcomes. It is becoming clear that the cardiologist needs both to consider T2DM in cardiovascular treatment decisions and potentially to help guide the selection of glucose-lowering medications. Our statement provides a comprehensive summary of effective, patient-centered management of CAD in patients with T2DM, with emphasis on the emerging evidence. Given the increasing prevalence of T2DM and the accumulating evidence of the need to consider T2DM in treatment decisions, this knowledge will become ever more important to optimize our patients’ cardiovascular outcomes.
Antiplatelet Therapy
Aspirin and Clopidogrel
Ticagrelor
Platelet Function Testing
Blood Pressure Control
Choice of Antihypertensive Agents
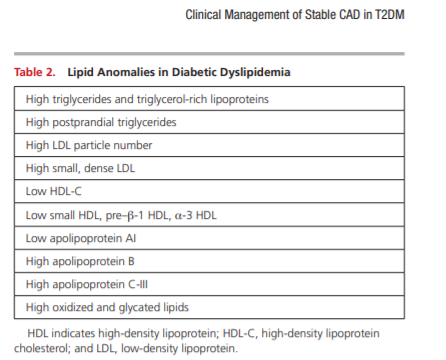
Lipid Management
Nonstatin LDL-C–Lowering Treatments
Non-LDL Target Therapies
Icosapent ethyl is the first non–LDL-focused lipid therapy to demonstrate cardiovascular benefit and should be considered first-line therapy for patients with T2DM and CAD whose triglycerides remain elevated (>135 mg/dL) despite maximally tolerated statin and lifestyle changes, as now recommended in the American Diabetes Association Standards of Medical Care.5
Lifestyle Modification and Weight Management
Start here.



