Note to myself and my readers: I’ve reviewed a number of resources both in my blog and on the internet on alcohol use disorder. And I’ll be reposting on them in the coming days. One resource I find outstanding is from emedicine.medscape.com – Alcoholism
Updated: Mar 23, 2020
Author: Warren Thompson, MD, FACP:
Alcohol use is the fourth leading cause of preventable death in the United States (after smoking, high blood pressure, and obesity). According to a 2018 report from the WHO, in 2016 the harmful use of alcohol resulted in about 3 million deaths, or 5.3% of all deaths around the world, with most of these occurring among men. [1, 2] The economic costs of excessive alcohol consumption in 2010 were estimated at $249 billion, or $2.05 a drink. [3]
DIAGNOSE AND TREAT PATIENTS WITH RISKY DRINKING AND ALCOHOL USE DISORDER
Here is the podcast embedded:
Here are excerpts from the show notes:
We learn how to initiate medications such as naltrexone and acamprosate for the treatment of alcohol use disorder, how to define treatment success, if psychosocial interventions such as Alcoholics Anonymous are effective, and what’s the deal with baclofen and gabapentin? After listening to this episode, listeners will feel ready to start prescribing medications such naltrexone to treat alcohol use disorder. Your patients need you!
Alcohol Use Disorder Pearls
Risky drinking is defined as more than 4 drinks per occasion or more than 14 drinks a week for men. For women the criteria are defined as more than 3 drinks an occasion, or more than 7 drinks a week.
Screen all adults in the primary care setting for risky drinking with one of the following 3 validated tools: AUDIT, AUDIT-C and the single question screen (How many times in the past year, have you had 4 or more drinks in a day (for women), or 5 or more drinks (for men)?
Motivational Interviewing tip: Use your OARS – Open ended questions, affirmations, reflective statements, and summarizing.
To help remember some of the DSM-V criteria for AUD break them up into their physiologic symptoms, a) withdrawal b) tolerance and c) the 5 C’s: loss of Control, Cravings, health and relationship Consequences, Compulsion to drink, and being unable Cut back.
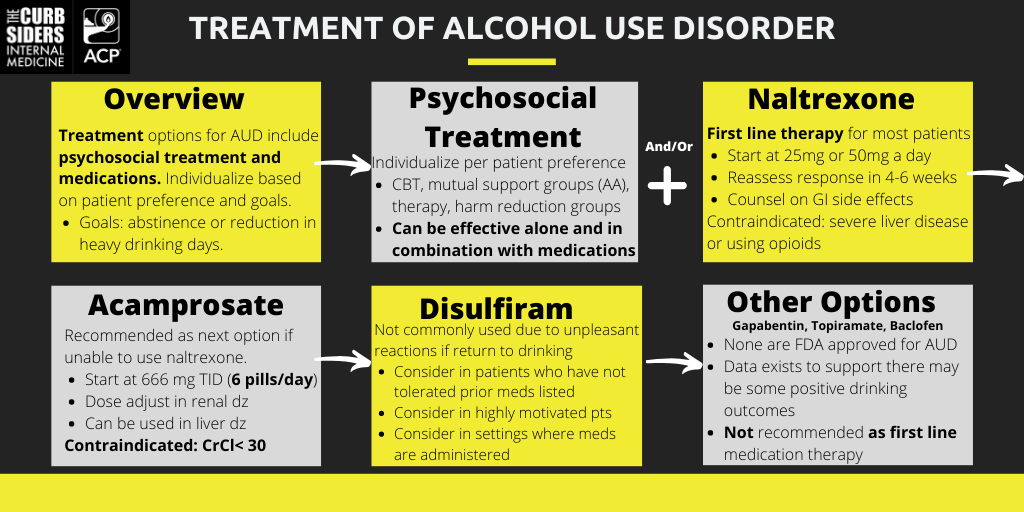
FDA approved medication treatment for AUD includes naltrexone PO, naltrexone LAI (long acting injectable formulation), acamprosate, and disulfiram.
Keep in mind the patient’s comorbidities when selecting a pharmacologic treatment option. Naltrexone is contraindicated in severe liver disease and in individuals who use opioids. Acamprosate is contraindicated in CrCl < 30, and a patient must be motivated to have adherence to daily disulfiram.
Initiate naltrexone at either 25mg PO daily on day 1 (expert opinion, to minimize side effects), and 50mg on day 2. Follow-up to assess a patient’s success in cutting back and/or abstinence in 4-6 weeks.
These meds work! For naltrexone the NNT* is 12 for return to heavy drinking, 20 for return to any drinking (Jonas, 2014).
There is some evidence to suggest gabapentin, topiramate, and baclofen may help patients cut down on their number of heavy drinking days, but these medications should be considered only if the first line medications are not an option.
Psychosocial interventions may work as well as medication treatment. Any of them can be the right one, tailor the referral based on patient preference. Options include: mutual support groups (AA), harm reduction groups, therapy (individual, family, CBT), and contingency management.
Treatment Options for Alcohol Use Disorder based on The Curbsiders #194 Alochol Use Disorder with Marlene Martin MD. Graphic by Carolyn Chan MD.
Alcohol Use Disorder Show Notes
Spectrum of Alcohol Use
Alcohol use is a spectrum that ranges from abstinence and/or low-risk alcohol use to severe alcohol use disorders. The spectrum range is as follows: abstinence, low-risk alcohol use. From there it turns into a category of unhealthy alcohol use which is a continuum that ranges from: risky drinking to mild-severe alcohol use disorder (Saitz, 2005).
Defining Risky Alcohol Use
For men, risky drinking is defined as more than 4 drinks per occasion or more than 14 drinks a week. For women, risky drinking is defined as more than 3 drinks an occasion or more than 7 drinks a week (NIAAA, 2005).
Is consuming any amount of alcohol safe?
Dr. Martin’sdoes not recommend that any of her patient initiate drinking alcohol strictly for health benefits -expert opinion.
Screening for unhealthy alcohol use – “CAGE is dead”
USPSTF recommends that all adults in the primary care setting are screened for unhealthy alcohol use —USPSTF, site updated 2018. Mot screening tools have been validated in the outpatient setting, and are better when they are self-administered. The three tools the USPSTF recommends are AUDIT*, AUDIT-C and the validated single alcohol screening question (SASQ). Note*: If utilizing the full AUDIT (10 questions) to screen for unhealthy alcohol use then use a lower cutoff score of 3-5, to balance the to balance sensitivity and specificity
CAGE is no longer recommended as a first line screening tool for alcohol use disorder.
Validated Single Question Screen
Start with a validated single question which screens individuals for unhealthy alcohol use: How many times in the past year, have you had 4 or more drinks in a day (for women), or 5 or more drinks (for men)? If a patient answers “yes” to the question, then they have screened positive for unhealthy alcohol. This single item question has been validated, it is 82% sensitive, and 79% specific for identifying patients with risky alcohol use (Smith, 2009).
Diagnosing Alcohol Use Disorder
DSM-V is the gold standard in diagnosing alcohol use disorder*. If a patient meets 2-3 criteria they a mild AUD, 4-5 criteria is a moderate AUD, and 6 + is a severe AUD (DSM-V, 2013).
The FDA has approved 4-first line pharmacologic agents for the treatment of AUD which include: naltrexone PO, naltrexone long acting injectable (LAI), acamprosate, and disulfiram. In Dr. Martin’s opinion, naltrexone and acamprosate are her go-to first line agents.
INITIATING NALTREXONE – START TOMORROW, YOUR PATIENTS NEED YOU!
Day 1: Start naltrexone at 25mg (expert opinion to minimize side effects), and then increase to 50mg on day 2. Alternatively some providers may start 50mg on day 1 and continue this dose.
Common side effects include abdominal pain, nausea, vomiting, and diarrhea. Dr. Martin prefers to start at 25mg to minimize side effects, which often dissipate with time. It can be started at a dose as low as 12.5mg for 7 days if an individual has experienced adverse side effects in the past (Chapter 4: Oral Naltrexone SAMHSA/CSAT, 2009). For medication titration, assess if the patient has cut back successfully on their alcohol use while on naltrexone. If they have and would like to try to cut back further, consider increasing the dose up to 100mg daily, after 4-6 weeks.
Consider extended release naltrexone (injection) for individuals who have trouble adhering to the pill formulation. Of note the injectable formulation is expensive.
Acamprosate
Acamprosate is a glutamate antagonist that helps patients in the protracted symptoms of alcohol withdrawal that often lead people to drinking. It is good for individuals who experience dysphoric effects when they stop drinking such as insomnia.
INITIATING ACAMPROSATE
It’s simple to initiate, but a large pill burden for patients. The starting dose is 666 mg TID (six 333 mg pills per day!). Of note, it must be renally dosed. If CrCl < 50, reduce the dose to 333mg TID, and if CrCl < 30 the medication is contraindicated. In contrast to naltrexone, this medication can be used in patients with end stage liver disease —Chapter 2: Acamprosate SAMHSA/CSAT, 2009.
Disulfiram
Disulfiram is FDA approved for the treatment of AUD but is not commonly used. Often individuals do not take it because they have unpleasant reactions if they return to drinking. Dr. Martin’s expert opinion is to consider it for those who have not tolerated naltrexone or acamprosate, yet are highly motivated to quit drinking. In addition, one can consider in patients who are in settings where the medication is administered, such as patients going to daily methadone clinics where disulfiram could also be given.
Patients with co-occurring opioid use disorder or depression
Assess which disorder is the patient’s main substance use disorder. For example, if alcohol use disorder is the main disorder (ie patient drinks daily, but uses opioids sporadically), consider trialing acamprosate for treatment of their AUD. Naltrexone is contraindicated in individuals with opioid use disorder (OUD) or chronic opioid use. While LAI naltrexone is FDA approved to treat both, it is often not the first line for OUD. Dr. Martin would only consider LAI naltrexone for patients with co-occurring disorders who do not want to try buprenorphine-naloxone or methadone.
A Cochrane review suggests if a patient has depression and co-occurring AUD, consider offering the patient an SSRI. When started on an SSRI there is low quality evidence to support that patients may have a reduction in their alcohol consumption (Agabio, 2018)
[Personal thought: I would use an SSRI for anxiety.]
Here are links to resources to some mental health screening instruments: