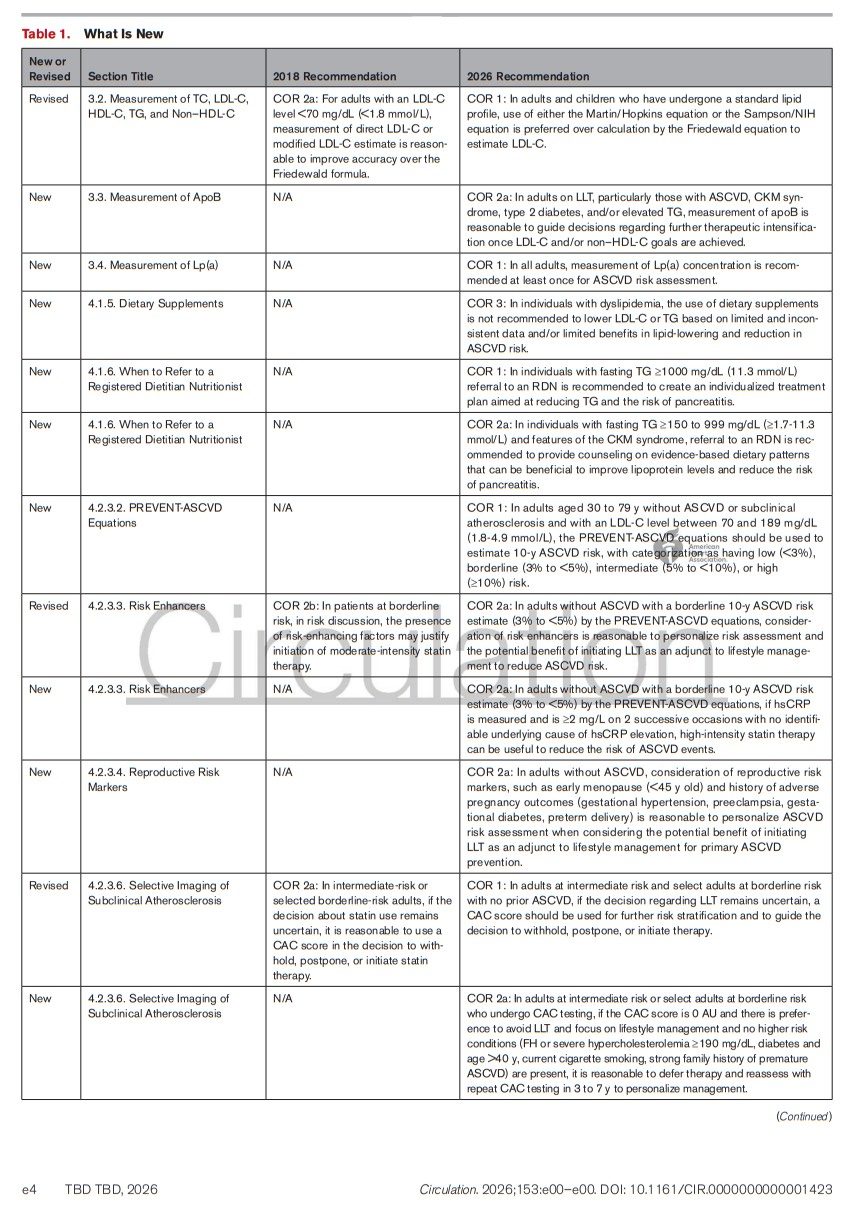
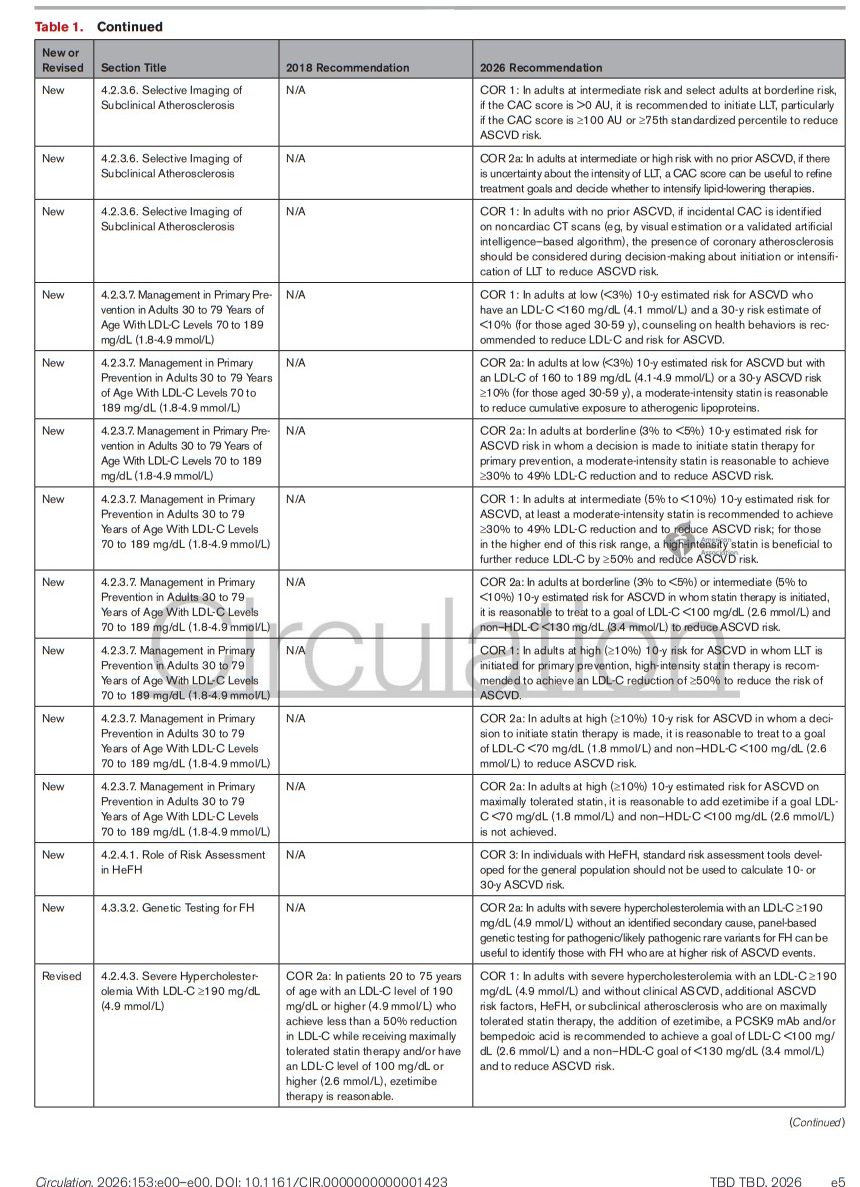
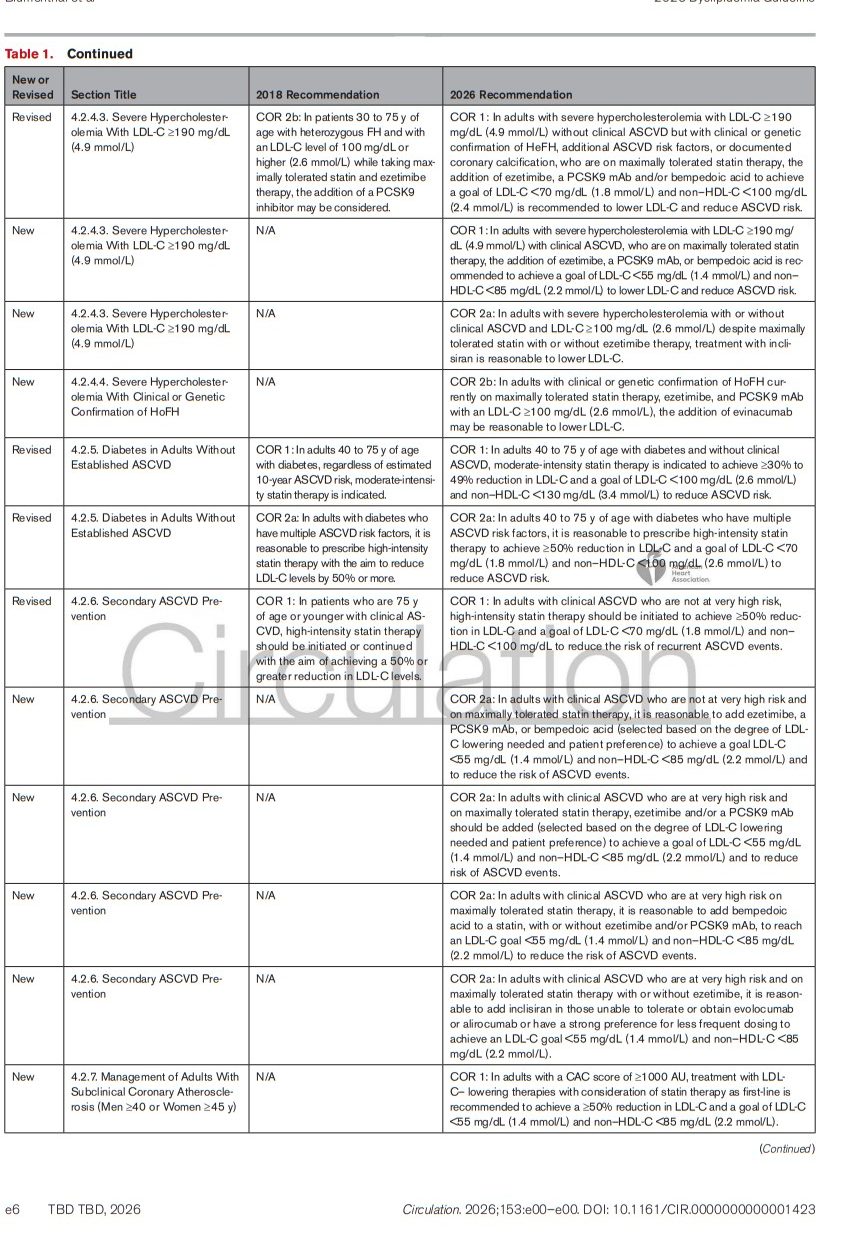
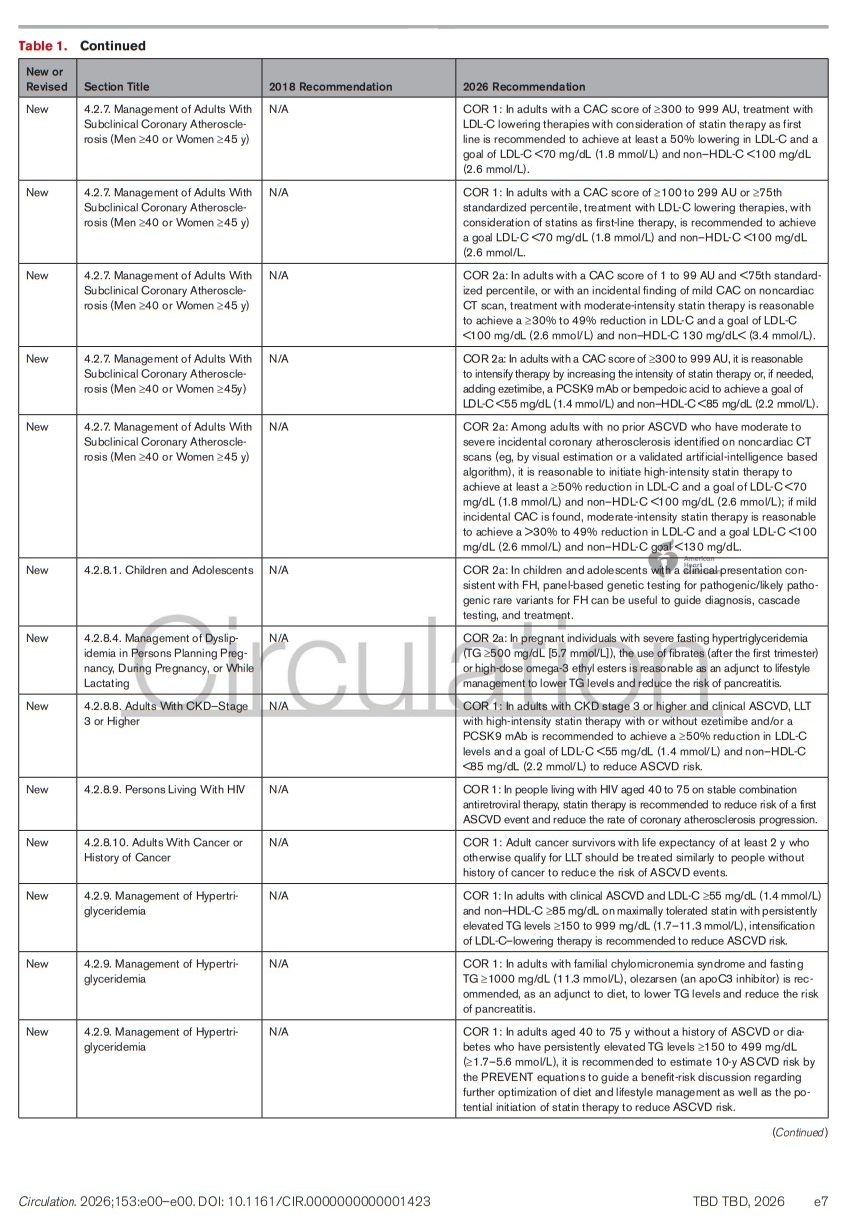
Today, I review, link to, and excerpt from What’s New [Table 1] in the “2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Circulation. 2026 Mar 13. doi: 10.1161/CIR.0000000000001423. Online ahead of print.
All that follows is from the above resource.