
In addition to today’s resource, please review:
Linking To And Excerpting From “The ketogenic diet is not for everyone: contraindications, side effects, and drug interactions”
Posted on February 18, 2026 by Tom Wade MD
Today, I link to and excerpt from Frontiers In Nutrition‘s Awareness and best practices in using ketogenic therapy to treat serious mental illness: a modified Delphi consensus. [Full-Text HTML] [Download PDF]. ORIGINAL RESEARCH article: Front. Nutr., 23 February 2026. Sec. Nutrition and Metabolism. Volume 13 – 2026 | https://doi.org/10.3389/fnut.2026.1749406
All that follows is from the above resource.
Abstract
Background:
Metabolic dysfunction is emerging as an important contributor to the pathophysiology of major depressive disorder, bipolar disorder, and schizophrenia, fueling interest in ketogenic metabolic therapy (KMT) as a potentially beneficial intervention for serious mental illness. KMT has been used successfully for decades in treating epilepsy, but evidence for treating mental illness has yet to mature.
Aims:
This study aimed to produce expert-informed guidance for the implementation of KMT in adults with serious mood and psychotic disorders.
Method:
A modified Delphi methodology was used to examine the opinions of KMT-experienced mental health experts. A steering group of eight such experts convened to develop an online survey comprising 33 statements regarding 1) the definition of KMT in the context of serious mood and psychotic illness; 2) identification of eligible candidates; 3) monitoring and measurement standards; and 4) best practices in employing KMT. This survey was distributed to clinician peers to examine opinions. The threshold for consensus agreement was set a priori at 75%.
Result:
Consensus was reached for all 33 statements (100%); therefore, the steering group approved the complete series of recommendations.
Conclusions:
This consensus provides expert-informed guidance to support the use of KMT in adults with major depressive disorder, bipolar disorder, and schizophrenia.
1 Introduction
Schizophrenia, bipolar disorder, and major depressive disorder afflict hundreds of millions of people globally (1) and are associated with poor quality of life, reduced life expectancy, and high socioeconomic burden (2).
Despite decades of prescription drug treatments designed to remediate underlying dysfunction in neurotransmitter systems, this approach continues to leave many individuals without meaningful relief (3). Those who do benefit from psychotropic drugs often suffer serious side effects that negatively impact quality of life, cause metabolic dysfunction, and can even be life-threatening (1, 2, 4, 5). Pharmaceutical innovation in psychotropic medication has essentially stalled, with few drugs with novel mechanisms of action approved in recent years (6). This lack of new and effective treatment options is particularly challenging for individuals whose conditions have not responded to multiple psychotropic drugs and are therefore considered treatment-resistant (3, 7–10).
For these reasons, the search for modifiable factors underlying serious mental illnesses has expanded beyond neurotransmitter system dysfunction to include neuroinflammation and excessive oxidative stress (both of which disrupt neurotransmitter production pathways), and insulin resistance—a common driver and marker of general metabolic dysfunction (11, 12). Serious mood and psychotic disorders are strongly correlated with metabolic disorders (13, 14). For example, people with glucose levels in the prediabetes range are 2.7 times more likely to develop major depression (15), those with newly diagnosed bipolar disorder are 3.5 times more likely to have metabolic syndrome (16); and individuals with newly diagnosed schizophrenia are 3.7 times more likely to have insulin resistance (17, 18). Insulin resistance is linked to cerebral glucose hypometabolism, which has been observed in schizophrenia, bipolar disorder, and treatment-resistant major depressive disorder (19). It has been demonstrated in a carefully controlled clinical trial that reversing insulin resistance with medication (metformin) may substantially improve depression symptoms in adults with treatment-resistant bipolar disorder (20), suggesting that addressing metabolic dysfunction by other means such as with lifestyle changes may also offer clinical benefits.
Ketogenic metabolic therapy (KMT), an intervention that leads to potentially therapeutic levels of ketone bodies in the blood, can improve metabolic health (18). While it is possible to lower insulin levels enough to initiate ketogenesis through fasting or significant caloric restriction (21), or raise circulating ketone levels using exogenous ketone (beta-hydroxybutyrate) supplements (11), the safest way to maintain ketosis long-term is with a ketogenic diet.
KMT has been shown to decrease neuroinflammation, regulate neurotransmitter systems, reduce hyperexcitability of the neural network, stabilize neuronal firing rates, and improve brain energy metabolism (11). Indeed, mitochondrial dysfunction is increasingly implicated in the pathogenesis of many neuropsychiatric disorders (22) including schizophrenia (23), bipolar disorder (24), and major depressive disorder (25). KMT improves brain bioenergetics by bolstering antioxidant defenses, which protects the health of existing mitochondria, and by promoting mitochondrial biogenesis, the creation of new mitochondria (26).
The clinical utility of KMT has been demonstrated in epilepsy for many decades (27), and a growing body of evidence that includes preclinical research and human case reports suggests a similar approach could improve both metabolic dysfunction and serious psychiatric symptoms, even supporting remission of treatment-resistant mood and psychotic illnesses in some cases (28, 29).
Although data from larger, more rigorous human clinical trials of KMT in serious mood and psychotic illnesses are not yet available, a growing number of clinicians have been turning to KMT in an effort to improve outcomes for patients living with these challenging conditions.
Our objective was to engage KMT-experienced mental health experts in a modified Delphi study to develop clear clinical guidance for the safe and appropriate implementation of KMT in the treatment of serious mood and psychotic illnesses.
2 Materials and methods
This study did not require registration because neither the assigned interventions nor the outcomes assessed were related to the health of participants.
The process followed a modified Delphi methodology (30) (Figure 1), a well-established approach to answering a research question through identification of a consensus view across subject experts (31). We developed statements which were subsequently circulated to an anonymous wider panel of stakeholders to consolidate current best practice into expert recommendations.
Figure 1
Modified Delphi study stages and objectives.
2.1 Literature review
We reviewed the literature on the topic of ketogenic therapy in mental illness in October 2023, using PubMed, Google Scholar, and clinical trial registration databases. Search terms included but were not limited to: “ketogenic therapy”, “ketogenic diet”, “ketosis”, “bipolar disorder”, “schizophrenia”, and “major depressive disorder”, and this was supplemented by a general web search using free text terms.
2.2 Steering group
We convened a steering group in November 2023 to discuss the principles and practicalities of using KMT in serious mood and psychotic disorders. The group comprised 8 mental health experts (5 clinical psychiatrists, 1 licensed mental health counselor, and 1 registered dietitian all based in the United States, and 1 metabolic psychiatry research fellow based in Scotland) and was guided by an independent facilitator (Triducive Partners). Selected panelists represented leaders in their respective core disciplines (psychiatry, nutrition, behavioral health, and clinical research) who had demonstrated a considerable degree of clinical, scholarly, and/or research experience specifically pertaining to the use of KMT in adults with bipolar disorder, schizophrenia, and/or major depressive disorder.
We developed key questions based on the literature review to drive the meeting discussion. The meeting focused on four broad topics:
- A The definition of KMT in the context of serious mood and psychotic disorders
- B Identification of optimal candidates for KMT
- C Measurement and monitoring standards for KMT
- D Best practices in employing KMT
Round 1: Working collaboratively, the group discussed each topic in turn and suggested 31 statements. The group then independently rated the statements as either “accept”, “remove”, “reword”, or suggested additional statements. Recommendations were accepted based on a simple majority.
Round 2: The resulting statements were developed into a Likert survey for distribution to a wider panel of peers in the group’s professional networks by email using a snowball method. Panelists were experienced mental health experts with knowledge of the use of KMT in practice. Round 2 responses were collected and aggregated by an independent facilitator (Triducive Partners). Although the survey was sent to known individuals to ensure appropriate expertise, responses were anonymized.
Stopping criteria were 1) a 3-month window to collect responses; 2) a target of 50 responses; and 3) 90% of statements passing the (widely accepted) consensus threshold of 75% (32).
A statement of consent was included at the start of the survey, and consent was implied by completion and submission of the survey. As this study only collected the anonymous opinions of mental health professionals, and no identifying or patient-specific data was captured, ethical approval was not required.
Responses were captured using Microsoft Forms technology by the independent facilitator. Panelists were not compensated.
Completed surveys were analyzed in April 2024 using Microsoft Excel software. Responses were aggregated to provide an overall agreement level (i.e., the number of respondents expressing agreement as a percentage of the overall number of responses for each statement). Two weeks later, the steering group reviewed the responses to determine how they guided the conclusions and recommendations to be put forward.
2.3 Patient and public involvement
None. The stated objective was to examine the opinions of mental health experts regarding the principles of KMT use in serious mood and psychotic disorders and provide clinical guidance for implementation.
3 Results
During Round 1, of the initial 31 statements, 5 were removed, 20 were reworded, and 7 new statements were added, resulting in a final agreed set of 33 statements (S1–S33).
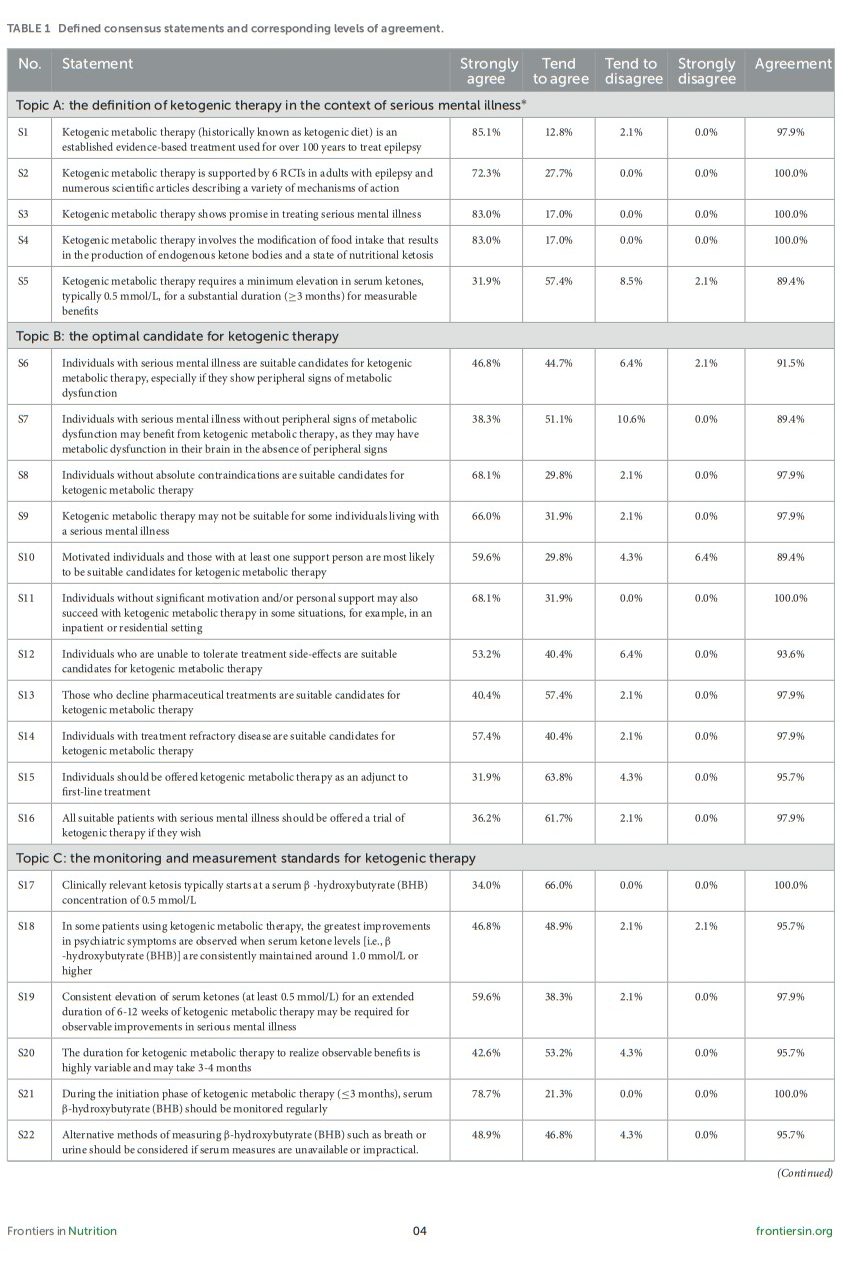
At the end of Round 2, 99 respondents initiated the survey, 52 of whom did not meet the screening criteria (i.e., did not currently work in the mental health field, reported no knowledge of ketogenic or metabolic therapies, or were not using ketogenic metabolic therapies in practice). The remaining 47 respondents completed the survey and were included in the analysis of results (Table 1). Respondents’ roles included physician (n = 24), psychologist (n = 1), dietitian (n = 8), health coach (n = 6), therapist (n = 5), nurse (n = 3), or a combination of these. The majority of respondents (37/47) had greater than 5 years of experience in their role, 13/47 respondents described their knowledge of ketogenic and other metabolic therapies as “very experienced/expert”, 27/47 as “some experience in practice”, and 7/47 as having awareness but not experienced in practice.
Table 1
As the stopping criteria were not satisfied, the steering group agreed to extend the window for collection for an additional month with the aim of achieving 50 responses. One appropriate additional response was received (47 responses total).
All statements achieved consensus agreement, with >91% of respondents strongly agreeing on 30/33 (91%) statements, and between 75% and 91% tending to agree on 3/33 (9%) statements (Table 1, Figure 2).
Figure 2
Consensus agreement levels by statement. The threshold for consensus is depicted by the green line (75%).
Figure 3
4 Discussion
Panelists reached consensus across all 33 statements. The steering group then used these statements to create the following recommendations, which can be used to inform key considerations for clinicians wishing to employ KMT in the treatment of major depressive disorder, bipolar disorder, and schizophrenia.
4.1 Topics
4.1.1 Topic A: The definition of ketogenic therapy in the context of serious mental illness
Respondents agreed that the ketogenic metabolic state should ideally be achieved through modifications of food intake that support the production of endogenous ketone bodies (S4, 100%), specifically by transitioning to a very-low-carbohydrate, adequate-protein, high-fat ketogenic diet. Ketogenic diets should be constructed to provide all essential nutrients, and the proteins and fats they contain may be animal-sourced and/or plant-sourced (33).
Respondents were aware of Level 1 evidence supporting the use of KMT in epilepsy (S1, 98%; S2, 100%) and agreed that there is clear potential for use in serious mental illness (S3, 100%). Respondents agreed that clinically relevant ketosis begins at 0.5 mmol/L beta-hydroxybutyrate (BHB), but that many individuals may require BHB levels of 1.0 mmol/L or higher for best outcomes (S5, 89%). Clinical response times are highly variable; respondents agreed that it may take several weeks to several months of consistent ketosis for measurable clinical benefits of KMT to manifest (S5, 89%; S19, 98%).
4.1.2 Topic B: The optimal candidate for ketogenic therapy
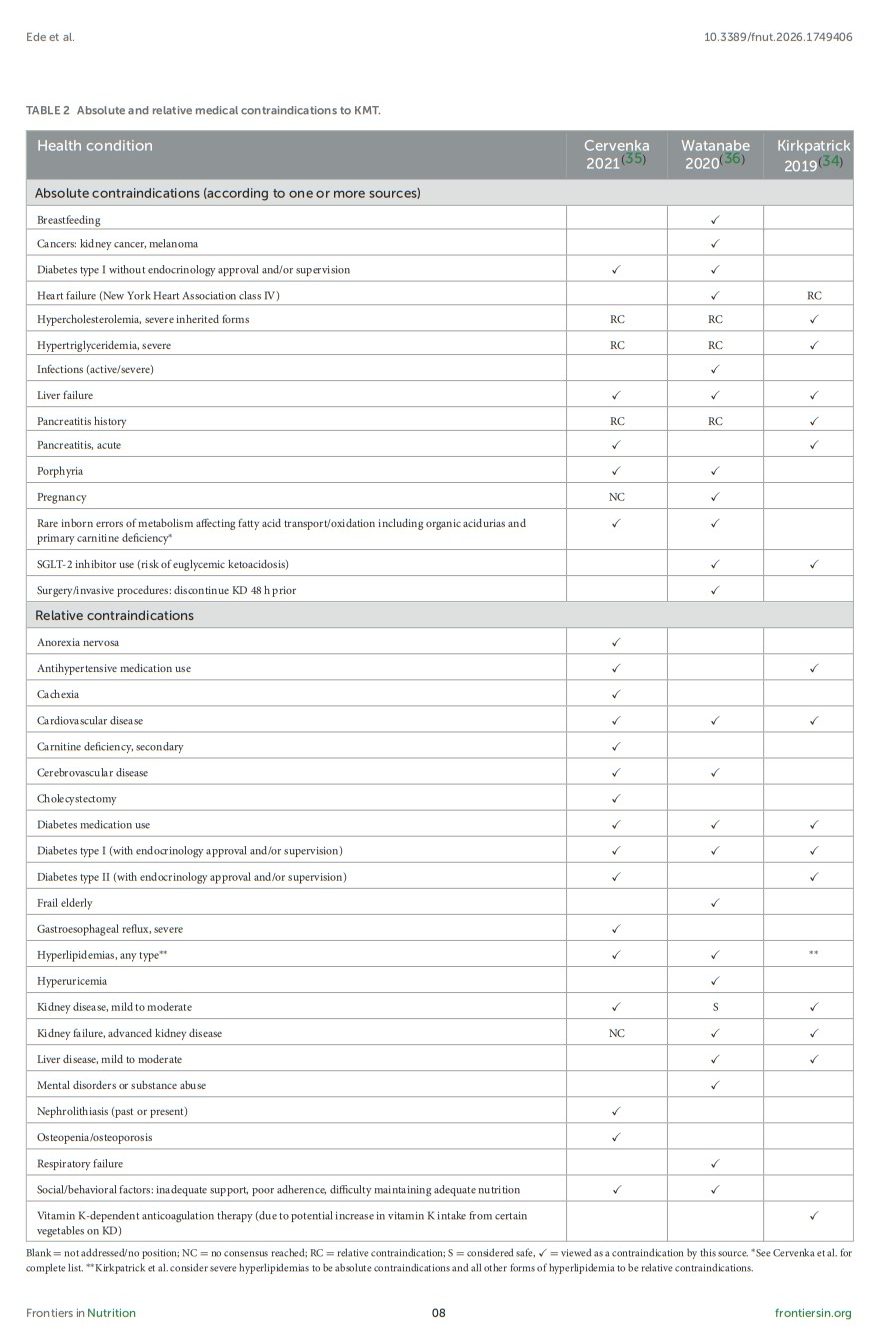
This topic was intended to identify adults with major depressive disorder, bipolar disorder, and schizophrenia who are most likely to benefit from KMT. Respondents agreed that a trial of KMT is appropriate for most adults with these serious mood and psychotic illnesses (S6, 91%; S7, 89%). However, there are a few absolute contraindications to be aware of that make proceeding with KMT potentially dangerous, and many relative contraindications that warrant careful consideration before deciding whether to initiate KMT (S9, 98%). For these reasons, a detailed medical and psychiatric history must always be taken prior to considering KMT.
Table 2 lists medical conditions viewed as absolute and relative contraindications to KMT according to three recent authoritative reviews (34–36). Expert opinions vary, most notably with respect to severe hypertriglyceridemia and hypercholesterolemia, which are viewed as absolute contraindications by the National Lipid Association (34) but as relative contraindications by other sources. Although there is mounting evidence that elevated LDL cholesterol does not pose a direct risk to cardiovascular health (37–40), the authors recommend caution in these cases, as the elevations in LDL cholesterol that sometimes accompany carbohydrate restriction could exacerbate pre-existing dyslipidemias.
Table 2
Where relative contraindications exist, skilled medical supervision or clinical guidance is required, for example during breastfeeding (41) and in type I and type II diabetes (42).
Although documented instances of clinically concerning psychiatric symptoms emerging, resurfacing, or worsening in the context of KMT implementation are rare, this may be due to the limited number of published cases and clinical trials in this young field to date. Given that it can take several weeks to several months for mental health benefits of KMT to manifest, the authors recommend that KMT not be used as a standalone intervention for acute, unstable, or potentially dangerous psychiatric presentations such as new or worsening mania, new or worsening psychosis, active suicidal ideation, self-injurious behavior, severe agitation, aggressive behavior, intoxication, or mental status changes. The absence of published clinical experience in cases such as these is yet another reason to caution against the use of KMT as a primary intervention. Even when considering a trial of KMT to help manage serious symptoms that have already been safely stabilized, additional safeguards may be required such as specialist consultation, medication support, intensive outpatient treatment, residential care, or inpatient hospitalization.
Comorbid psychiatric conditions such as substance use disorders (e.g., alcohol and other drug use disorders) and advanced cognitive impairment should also be taken into consideration during treatment planning. Finally, although KMT is being explored as a potentially therapeutic adjunctive tool in the management of residual eating-disordered thoughts and behaviors in people with weight-recovered anorexia nervosa (43), the authors currently view underweight anorexia nervosa as an absolute contraindication to KMT.
Respondents agreed that, outside of an absolute contraindication, KMT should be considered as an adjunct therapy to first-line treatments such as psychotropic medications and psychotherapy for all individuals with serious mood and psychotic illnesses (S8, 98%), including:
- Individuals with treatment-refractory serious mood and/or psychotic illness (S14, 98%)
- Individuals who do not tolerate pharmaceutical treatments (S12, 94%)
- Individuals who do not wish to use pharmaceutical treatments (S13, 98%)
- Individuals with peripheral signs of metabolic dysfunction (S6, 91%)
- Individuals who wish to undertake a trial of KMT (S16, 98%)
The likelihood of success of KMT increases when support is in place (S10, 89%). Individuals with less motivation or support may benefit from an intensive outpatient, residential, or inpatient care setting (S11, 100%).
KMT (by definition) is intended to address metabolic dysfunction and is therefore recommended for individuals who exhibit one or more signs of metabolic dysfunction (S6, 91%). These include elevations in fasting glucose, hemoglobin A1c, fasting insulin, triglycerides, triglyceride-to-HDL ratio, blood pressure, and waist-to-height ratio (a measure of central obesity). Even when observable signs of peripheral metabolic dysfunction are absent, KMT is still worth considering, as metabolic dysfunction may still be present in the central nervous system (S7, 89%) (44, 45).
In cases where KMT is not appropriate, feasible, or desired, personalized nutrition counseling focused on improving overall dietary quality may bring metabolic and mental health benefits and is therefore well worth considering; however, an evaluation of specific dietary strategies other than ketogenic dietary therapy was not conducted by the steering group as it was beyond the scope of this endeavor.
4.1.3 Topic C: The monitoring and measurement standards for ketogenic therapy
The authors recommend that initial assessment include a complete blood count (CBC), comprehensive metabolic panel (CMP), fasting lipid profile, fasting insulin, vitamin B12, vitamin D3, and a carnitine panel (S23, 94%). They further recommend that these parameters be monitored regularly during KMT (S24, 100%) and that any nutrient deficiencies be addressed with supplementation (S25, 98%). Additional testing should be tailored according to each specific case.
The steering group did not establish consensus views on the specifics of carnitine assessment and replacement in the management of serious mental illness,* [Emphasis added] as experience and evidence in this area is limited. However, guidelines for the management of adults with epilepsy support supplementation if levels are low or if symptoms associated with carnitine deficiency are present (35). Carnitine is a conditionally essential nutrient responsible for transporting long-chain fatty acids into mitochondria in preparation for oxidation. If endogenous synthesis (from lysine and methionine) or exogenous supply (from dietary sources) of carnitine is insufficient to meet this increased demand, fat metabolism and ketone production could be compromised, resulting in lower than expected BHB levels and potentially also indicators of energy deficit, such as fatigue, hypoglycemia, or cognitive difficulties. Indeed, reductions in carnitine levels are not uncommon in adults following a KD for the management of epilepsy, and lower levels may be associated with poorer seizure control (46).* [Emphasis added]
Risk factors for acquired carnitine deficiency that make close monitoring especially important include use of valproate, liver disease, kidney disease, diets low in carnitine, lysine, and/or methionine (including vegan and vegetarian diets), malnutrition, type II diabetes, advanced age, and use of cyclosporin or pivampicillin (47–49). If free plasma carnitine is below 25 μmol/L, acetyl-L-carnitine in divided doses of up to 100 mg/kg per day as tolerated may be useful. As carnitine bioavailability from supplements is far lower than from foods, dietary counseling may also be worthwhile.* [Emphasis added]




* Google Search: what is a carnitine panel?



