Today, I review and excerpt from the Exit Section of
The “5Es” of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Acad Emerg Med. 2015 May;22(5):583-93. doi: 10.1111/acem.12652. Epub 2015 Apr 22.
All that follows is from the above resource.
While gross valvular abnormalities and intracardiac masses are important if they are seen, they are less common and less acute and tend to be less immediately deadly than acute thoracic aortic disease, which accounts for more than twice as many deaths as abdominal aortic aneurysm rupture.51 [Emphasis added]
Exit
The fourth “E” in our protocol is for exit from the heart, or the assessment of the aortic root for thoracic aortic aneurysm, and thoracic aortic dissection (TAD). Aneurysmal disease of the thoracic aorta predisposes to aortic dissection.49 TAD is a time-dependent and potentially deadly disease process that can present silently or masquerade as a variety of clinical presentations. TAD results from a tear in the intima of the aorta that can propagate in either an anterograde or a retrograde fashion. Retrograde dissections can produce a number of US findings such as an intimal flap, aortic valve insufficiency, retrograde aortic flow, or rupture into the pericardium with pericardial effusion and tamponade. While contrast enhanced computed tomography (CT) remains the test of choice for diagnosing thoracic aortic disease, transthoracic echo has been shown to be accurate for detection of aortic root dilation and may be performed rapidly with a high degree of specificity by the EP at the bedside in a patient presenting with acute chest pain and/or hemodynamic instability.7, 50
Techniques for Assessing Exit
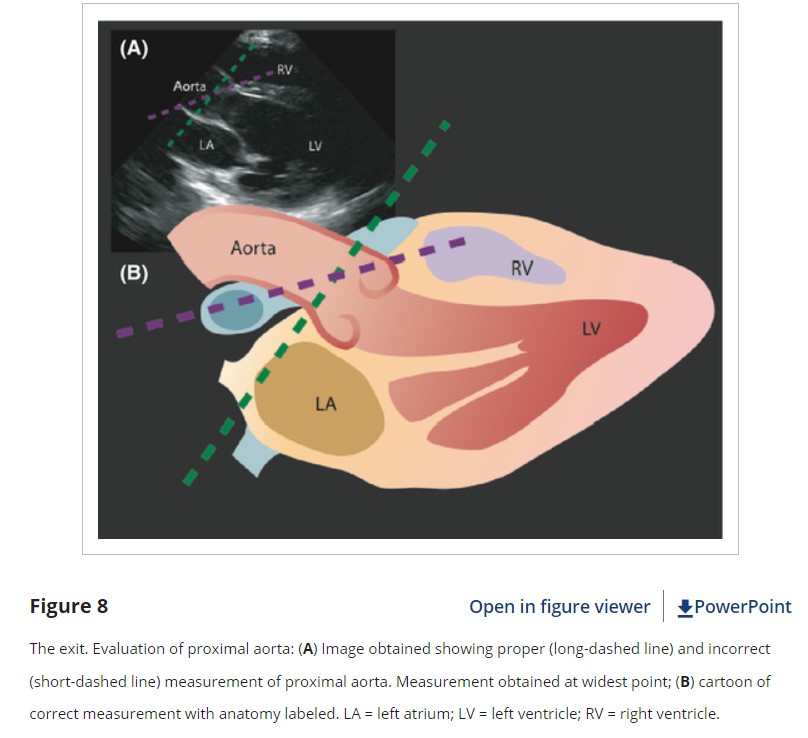
The proximal aortic root is best assessed using a PSLA window, and EP measurement of the aorta in this view correlates well with measurements on CT angiogram (CTA).7 The aortic root should be measured from leading edge to leading edge (outside wall to inside wall) at the widest visible point during diastole, which is typically across the sinuses of Valsalva (Figure 8). A thoracic aortic root of over 4.5 cm is typically considered aneurysmal. However, measurement on CTA may be slightly lower than measurements on echo, probably due to the angle of measurement.7, 49 For EP FOCUS, we recommend that measurements of <4 cm be considered normal, 4.0 to 4.5 cm borderline, and >4.5 cm aneurysmal.
With respect to aortic dissection, dynamic images of the ascending aorta may detect an intimal flap seen as a hyperechoic linear structure within the aortic lumen that moves with each heartbeat. While the sensitivity of TTE for intimal flap is low, its visualization carries a high specificity.50 Furthermore, a retrograde flap may cause aortic insufficiency and/or bleeding into the pericardium. The presence of aortic root dilation and/or intimal flap with a pericardial effusion should prompt immediate consultation to cardiothoracic surgery, with CTA if the patient will tolerate it.
Pearls and Pitfalls of Exit
A common error occurs when practitioners place their measurement cursors parallel to the edge of the US footprint rather than perpendicular to the long axis of the vessel. This results in oblique measurements that can overestimate the true aortic diameter (Figure 8).
While the “exit” of EP FOCUS reliably assesses the proximal aortic root, thoracic aortic dilatation or an intimal flap may occur distal to the aortic root. Assessment of other parts of the thoracic aorta may be enhanced by using a suprasternal notch window and by visualizing portions of the descending aorta, often seen in the far field on the PSLA view.
Mirroring and reverberation artifacts can mimic intimal flaps.51 To avoid errors in interpretation of intimal flaps, the examiner should interrogate the aorta from multiple angles and transducer locations, look for flap motion independent of surrounding structures, ensure that the structure is confined to the lumen, and use Doppler to demonstrate differential flow on either side of the flap.
Thoracic aortic dilatation is strongly associated with dissection; however, there can be aneurysm without dissection and dissection without aneurysm.49 The presence of thoracic aortic dilatation should prompt greater suspicion of thoracic aortic disease, but its absence should not rule it out. If there is suspicion of disease, CTA remains the diagnostic test of choice, particularly if the patient is hemodynamically stable. Early EP FOCUS may prompt and expedite appropriate diagnostic testing and consultation when needed.50
Conclusions
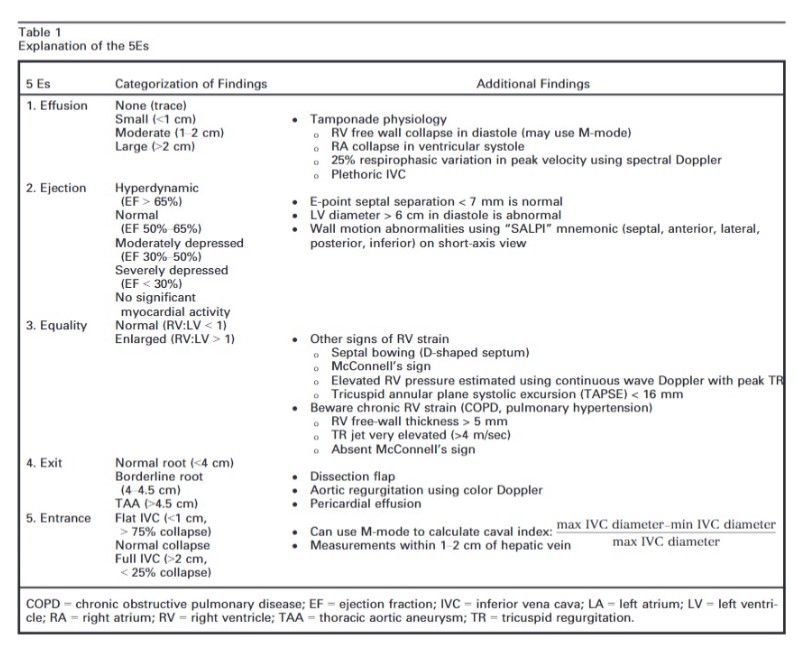
The intent of this article is to codify elements of the cardiac US exam that we have found to be most relevant to patients presenting with acute or emergent complaints (Table 1). A recent international consensus statement defined FOCUS as being goal-directed, problem-oriented, limited in scope, simplified, time-sensitive and repeatable, qualitative and semiquantitative, performed at the point of care, and usually performed by clinicians.6 The 5Es described in this article meet all of these criteria. However, the international statement addressed the use of FOCUS in “all clinical settings” and included the assessment of chronic cardiac disease, as well as gross valvular abnormalities and large intracardiac masses, without assessment of the thoracic aorta.
In our experience the 5Es encompass the cardiac US findings most applicable in patients who present emergently with hypotension, dyspnea, syncope, penetrating thoracic trauma, chest pain, or other acute complaints where diagnosis may be aided by visualization of the heart. While gross valvular abnormalities and intracardiac masses are important if they are seen, they are less common and less acute and tend to be less immediately deadly than acute thoracic aortic disease, which accounts for more than twice as many deaths as abdominal aortic aneurysm rupture.51The 5Es are not meant to provide an absolute boundary for EP FOCUS, which will likely continue to evolve, but are intended to provide a framework for the acquisition and interpretation of the most relevant and applicable components of echocardiography in the emergent setting. We hope that adoption and subsequent application of the 5Es in EDs will help to standardize and effectively teach the echo findings that may allow EPs to save lives and expedite the care of patients with potentially life-threatening illness.We thank Jane Hall, PhD, for preparing Figures 4, 6, and 8. We also thank Daniel Wadsworth Groves, MD, for manuscript review.