
In the EmCrit vidcast Podcast 185 – Disruption, Danger and Droperidol by Reub Strayer
October 31, 2016 by Scott Weingart, Dr. Strayer* discusses and gives guidance on the management of the three different types of acutely agitated patient:
- The patient who is agitated but cooperative
- The patient who is disruptive but without danger to himself or others.
- The patient with excited delirium who is [or may be] a danger to himself or others.
In addition to his vidcast below, Dr. Strayer posts his slides [This link is to Slideshare] which can be cycled through for a rapid review of his talk. I have included some of the slides so that I can quickly review aspects of Dr. Strayer’s talk.
You need to get the agitated potentially dangerous patient sedated using IM sedation through the clothing. And the sites, depending on what is available to you, include the anterolater thigh, the upper outer quadrant of the buttocks, or the deltoid.
Never endanger the staff by trying to start an IV in the above patient until he is adequately chemically restrained.
*Dr. Streyer has his own outstanding Emergency Medicine blog at Emergency Medicine Updates. This site is rich in great resources for any clinician charged with acute patient care. My favorite resource is his EM Cards [this link is to a complete list of all the EM Cards]. There are 1412 EM Cards covering almost every aspect of emergency and acute care. You can access any topic covered by an EM Card by typing the subject into the search box.
Here are some points from Dr. Streyer’s lecture:
There are 3 types of emergency department agitation:
- Agitated but cooperative
- Disruptive but not dangerous
- Excited delirium that is dangerous to the patient or others
For the agitated but cooperative patient who responds to suggestion and where there is no concern that the pt has a dangerous condition, have someone sit with them or give small dose of oral benzodiazepine.
Agitated but cooperative
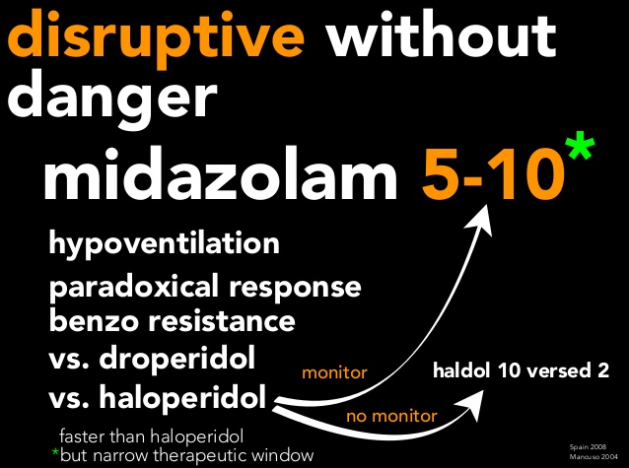
For the patient who is disruptive but conversant without being a danger to himself or others and where there is a low concern for a dangerous medical condition, the patient can be allowed to sleep it off.
Disruptive but not dangerous
For the patient who is disruptive but not dangerous to himself or others and who does not have a dangerous medical cause of his behavior, you can treat with:
- haldol 5 mg IM and lorazepam 2 mg
- droperidol 5 – 10 mg IM
- droperidol is the safest and best agent but for a number of reasons is no longer available in the United States.
- midazolam 5 – 10 mg IM
- If you use this option you need to monitor the patient according to the slide below.
- haldol 10 mg and midazolam 2 mg IM
- If you use this option you don’t [necessarily] need to monitor according to the slide below.
Excited delirium
Excited delirium is where the patient is a danger to himself, or to others, and/or is suffering from a dangerous medical condition.
Is the patient [just] disruptive versus delirious?
Err on the side of treating the patient as having excited delrium.
Don’t fight to get the vital signs but rather get the patient safely chemically restrained and then get the vital signs.
How to manage excited delirium:
- Have adequate force before approaching the patient
- Put face mask oxygen on the patient regardless of the patient’s position. It supplies oxygen and prevent spitting.
- Relieve dangerous restraint holds.
- Use chemical restraint not physical restraint. Until you get the patient sedated and under control:
- The clock is ticking
- The danger to the patient and or staff is unaddressed.
So focus on sedation.
And the key in chemical restraint is speed and safety. This means give the medication IM not IV. And give the medication through the clothes.
In chemical restraint, speed and efficacy trump concern for over-sedation (meaning respiratory depression).
[If you end up] intubating the excited delirious patient [this] is good care.
Your best medication for chemical restraint is rapid single shot IM ketamine.
You might say ” but this patient has an elevated HR and BP”.
No problem. Ketamine will normalize hyperdynamic vitals in most cases.
This is procedural sedation and requires PSA monitoring.
The dose of ketamine is 4 – 6 mg IM. Or just give 500 mg [Check lecture]
As the patient calms, continue to hold the patient but don’t use tight restraints. If the patient is in tight restraints, loosen them.
Loose restraints are okay but should be unnecessary and should not be necessary.
[Elevate] head of the bed.
As soon as the patient is chemically restrained you need to go to:
- 5. Get vitals – temp, fingerstick glucose, and a room air saturation or capnography.
- 6. Get vascular access and give a crystalloid bolus.
- 7. Identify and treat the dangerous causes and effects of severe agitation:
- First consider
- hypoxia
- hypothermia
- hypoglycemia
- hypoperfusion
- Second consider
- hyperkalemia
- acidemia
- ICH
- CNS infection
- Third consider
- sedative withdrawl
- serotonin syndrome
- NMS
- thyrotoxicosis
- sepsis
- seizure/postictal
- Na, K, Cr, NH3
- CK, trauma
- First consider
And finally we need to consider ongoing care, and here is Dr. Strayer’s slide on this topic and the last slide of his lecture:




