
The following slides are from Reference (1) below:
Text:
Text
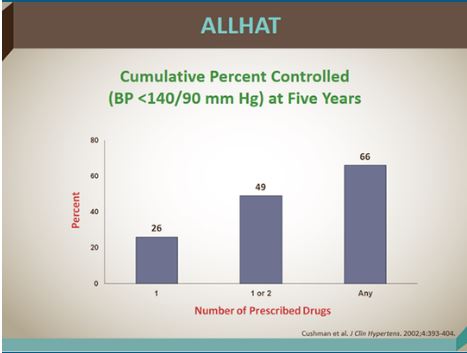
ALLHAT [Slide Below] showed that half of all hypertensive patients needed three or more drugs to get the blood pressure to less than 140/90.
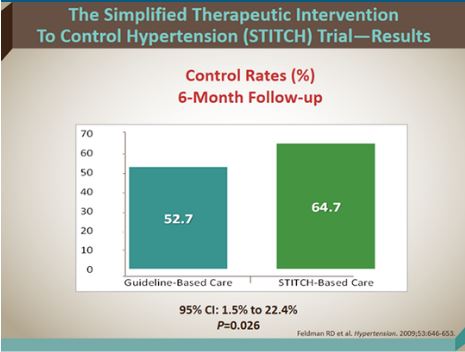
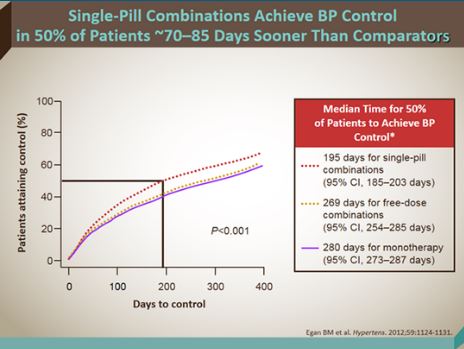
Fixed dose therapy is better than titrating a bunch of different single dose meds in terms of getting to goal. Compliance is higher and clinician therapeutic inertia is less. See results of the STITCH trial [Next two slides below]. Using the STITCH algorithm (starting with fixed dose combos) was more effective than the individual dosing CHEP Algorithm.
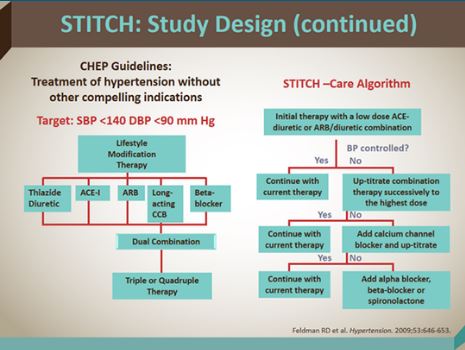
STITCH algorithm [Slide below] won and in real clinical practice it is likely that STITCH would be even more effective than usual practice (CHEP guideline)
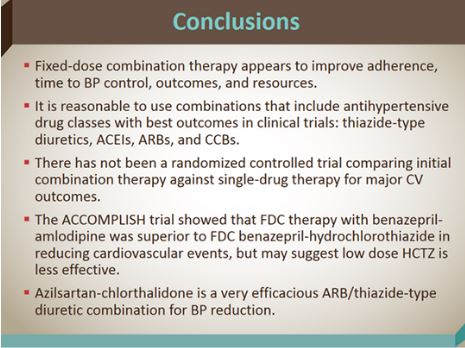
Bottom Line (Slide below):
Bottom Line Again (slide below)
You should only use beta-blockers if there are specific indications for a beta-blocker (for example, post-MI or pt with CHF). [The other classes are more effective at preventing hypertension complications.]
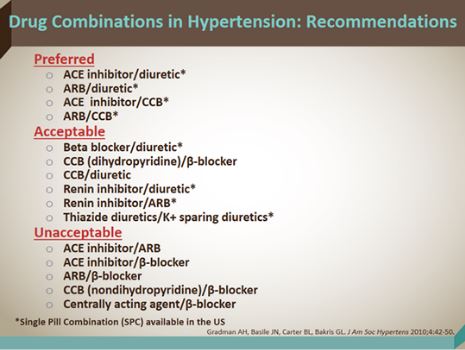
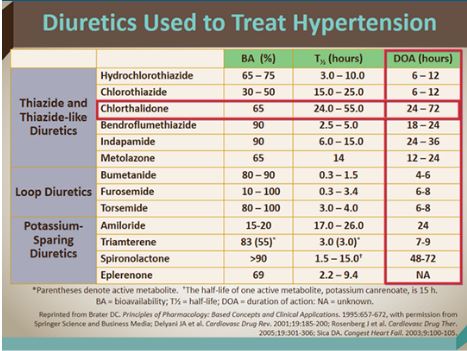
There are differences within classes and Dr. Cushman states that chlorthalidone is a more effective than hydrochlorothiazide ( even though hydrochlorthiazide is far more popular in the US).
Resources:
(1) Hypertension 2015: Important Concepts in BP Control CME 12-15-2015 from Medscape
Can BP Target Less Than 120 mm Hg Improve CV Outcomes? CME/CE 12-10-2015 from Medscape
The SPRINT Treatment Algorithm for the Intensive Treatment Group (Goal SBP < 120 mm Hg) – How They Did It. Posted on November 14, 2015 by Tom Wade MD
Ambulatory blood pressure monitoring in the diagnosis and management of hypertension.
[PubMed Citation] [Full Text HTML] [Full Text PDF]. Diabetes Care. 2013 Aug;36 Suppl 2:S307-11. doi: 10.2337/dcS13-2039.
Should 24-h Ambulatory Blood Pressure Monitoring Be Done in Every Patient With Diabetes? [PubMed Citation] [Full Text HTML][Full Text PDF]. Diabetes Care. 2009 Nov;32 Suppl 2:S298-304. doi: 10.2337/dc09-S326.



