
The following is from Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report [Full Text HTML] [Full Text PDF]. Chest. 2016;149(2):315-352. doi:10.1016/j.chest.2015.11.026:
AT9 = 9th Edition of the Antithrombotic Guideline
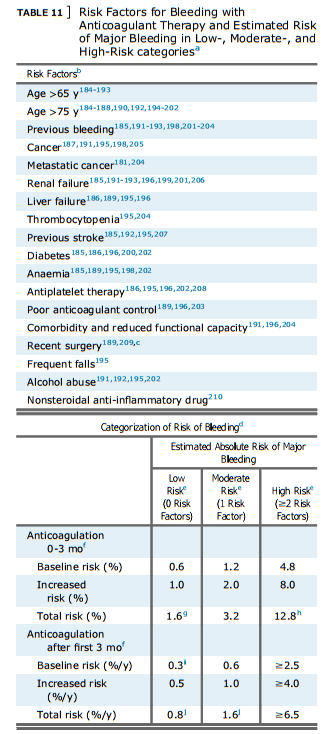
a From AT9. Since AT9, references for bleeding with individual factors have been added193,206,210; nonsteroidal anti-inflammatory drug has been added as a risk factor; a systematic review has described the risk in VTE trial patients who were randomized to no antithrombotic therapy211; and several recent publications have compared clinical prediction rules for bleeding in various populations.193,212-216
b Most studies assessed risk factors for bleeding in patients who were on VKA therapy. The risk of bleeding with different anticoagulants is not addressed in this table. The increase in bleeding associated with a risk factor will vary with: (1) severity of the risk factor (eg, location and extentof metastatic disease; platelet count); (2) temporal relationships (eg, interval from surgery or a previous bleeding episode197); and (3) how effectively a previous cause of bleeding was corrected (eg, upper GI bleeding).
c Important for parenteral anticoagulation (eg, first 10 d), but less important for long-term or extended anticoagulation.
d Although there is evidence that risk of bleeding increases with the prevalence of risk factors,187,188,192,194,195,196,198,201,202,204,217,218 the categorization scheme suggested here has not been validated. Furthermore, a single risk factor, when severe, will result in a high risk of bleeding (eg, major surgery within the past 2 d; severe thrombocytopenia).
e Compared with low-risk patients, moderate-risk patients are assumed to have a twofold risk and high-risk patients are assumed to have an eightfold risk of major bleeding.79,185,187,189,195,196,198,204
f We estimate that anticoagulation is associated with a 2.6-fold increase in major bleeding based on comparison of extended anticoagulation with no extended anticoagulation (Table 6 in AT91 ). The relative risk of major bleeding during the first 3 mo of therapy may be greater that during extended VKA therapy because: (1) the intensity of anticoagulation with initial parenteral therapy may be greater that with VKA therapy; (2) anticoagulant control will be less stable during the first 3 mo; and (3) predispositions to anticoagulant-induced bleeding may be uncovered during the first 3 mo of therapy.189,198,203 However, studies of patients with acute coronary syndromes do not suggest a higher than 2.6 relative risk of major bleeding with parenteral anticoagulation (eg, UFH, LMWH) compared with control.219,220
g 1.6% corresponds to the average of major bleeding with initial UFH or LMWH therapy followed by VKA therapy (Table 7 in AT91 ). We estimated baseline risk by assuming a 2.6 relative risk of major bleeding with anticoagulation (footnote f).
h Consistent with frequency of major bleeding observed by Hull in “highrisk” patients.209
i Our estimated baseline risk of major bleeding for low-risk patients (and adjusted up for moderate- and high-risk groups as per footnote e).
j Consistent with frequency of major bleeding during prospective studies of extended anticoagulation for VTE (Table 6 in AT91 ).64,65,80,189,221



