Additional Emergency Medicine Cases’ resources related to today’s post
- Jesse McLaren’s ECG Cases post on pericarditis for examples of differentiating pericarditis from MI and early repolarization
- PoCUS Cases pericardial effusion – technique and pitfalls
- 5 Minute Sono on pericardial tamponade
- Best Case Ever 31 on pericardiocentesis with Andrew Sloas
- NEJM emergency pericardiocentesis
- Ep 166 Pericarditis and Cardiac Tamponade
- Ep 167 Myocarditis – A Diagnostic Challenge
- Episode 163: Acute Heart Failure ED Management: Part I
- Episode 164: Cardiogenic Shock Simplified: Part II
In this post, I link to and excerpt from Emergency Medicine Cases‘ Ep 166 Pericarditis and Cardiac Tamponade.*
*Helman, A. Himmel, W. Dorian, P. Pericarditis and Cardiac Tamponade. Emergency Medicine Cases. March, 2022. https://emergencymedicinecases.com/pericarditis-cardiac-tamponade. Accessed 3-31-2022.
All that follows is from the above resource.
In this Part 1 of our two-part series on pericarditis and myocarditis, Anton is joined by Walter Himmel, EM doc at North York General and Paul Dorian cardiologist, researcher, and educator at St. Michael’s Hospital in Toronto (with a short visit from @ECG Cases Jesse McLaren). They answer questions such as: why should pericarditis be considered a diagnosis of exclusion? Which clinical features are most useful in the diagnosis of pericarditis? What are the most common pitfalls in the ECG interpretation of a patient suspected of pericarditis? What are the best ways to differentiate the ECG of pericarditis from that of MI and early repolarization? How is uncomplicated viral pericarditis treated differently compared to pericarditis of other etiologies? Why is it so important to include colchicine as part of the treatment of pericarditis? Which patients with pericarditis should be considered for admission? and many more…
Pericarditis as a diagnosis of exclusion
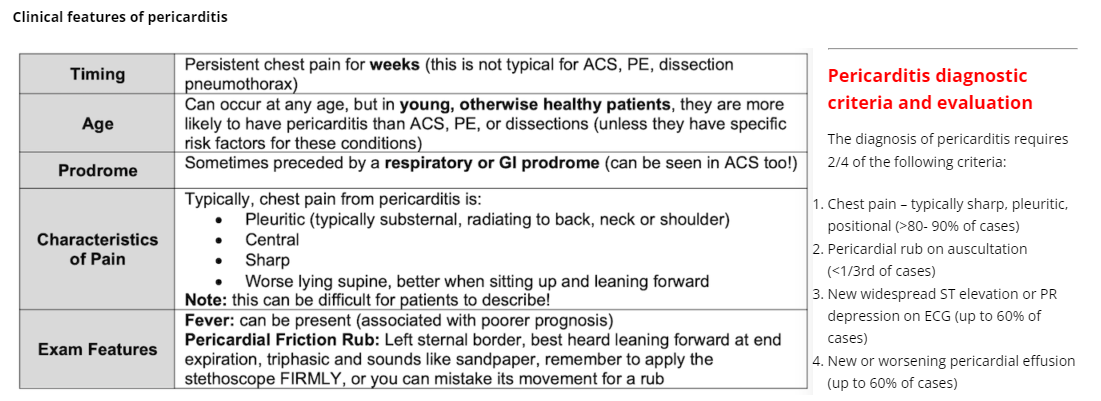
Pericarditis should be considered a diagnosis of exclusion, after ruling out the big chest pain killers (MI, PE, aortic dissection, esophageal rupture, and tension pneumothorax), because it can be easily confused with these more time-sensitive, deadly diagnoses. Avoid premature closure!
The following features are suggestive of pericarditis, but none alone have good enough test characteristics to rule it in or out.
Additional supportive findings:
- Elevated inflammatory markers (CRP, ESR, WBC count)
- Evidence of pericardial inflammation on imaging (contrast CT, cardiac MR)
Diagnostic evaluation for pericarditis
- Auscultate for friction rub (excellent specificity/poor sensitivity)
- ECG (see below)
- Ultrasound (see below)
- CXR (enlarged cardiac silhouette if associated with large pericardial effusion)
- WBC + diff – if very elevated consider bacterial cause such as TB and/or alternate diagnosis such as endocarditis
- ESR/CRP – thought to be useful to support diagnosis, risk stratify, assess effectiveness of treatment (serial evaluations) and predict recurrence
- Creatinine to asses for uremia as a cause
- Troponin to help rule out ACS and myopericarditis
Pearl: CRP it thought to be helpful in pericarditis diagnosis, risk stratification, assessing effectiveness of treatment through serial evaluations and predicting recurrence
ECG in pericarditis – more than just diffuse ST elevation
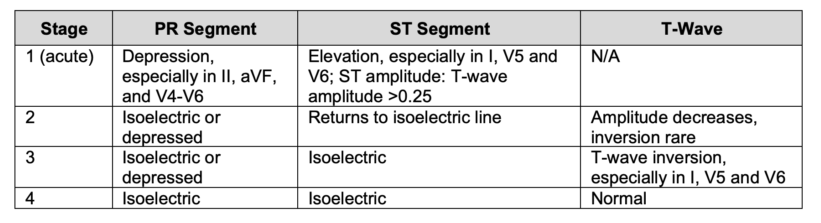
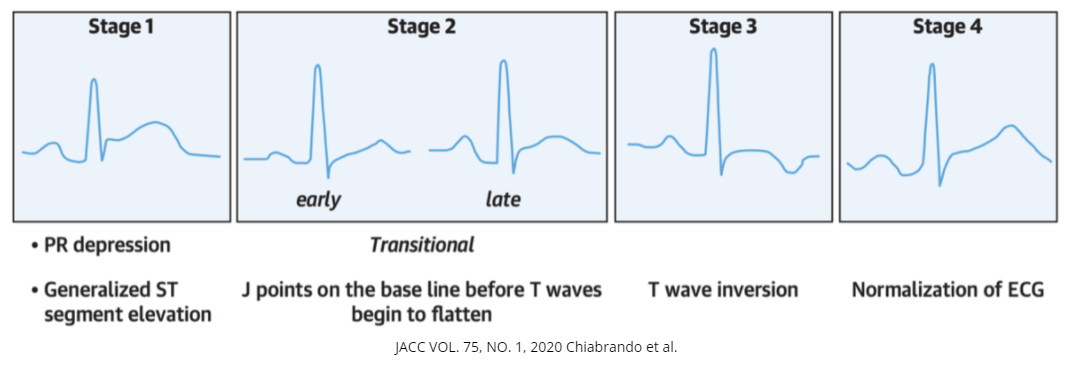
The 4 stages of ECG changes in pericarditis
It is important to understand that the classic diffuse ST elevation/PR depression (stage 1) is only found in 60% of patients with pericarditis as patients may present to medical care at a more advanced stage. The temporal evolution of the 4 changes are highly variable and some patients may skip directly from stage 1 to stage 4 (normalization).
Pitfall: An important pitfall in ECG interpretation is failing to consider MI in a patient with chest pain and diffuse ST elevation on ECG; diffuse ST elevation can occur in MI.
Pitfall: Some patients evolve directly from Stage 1 to Stage 4 (normalization) before they present to ED, so the ECG may be normal with acute pericarditis. Do not rule out pericarditis based on a normal ECG.
Pearl: Uremic pericarditis does not cause significant inflammation of the epicardium, so the ECG and the inflammatory markers are more likely to be normal.
ECG findings to help differentiate Pericarditis from MI
No single ECG finding is diagnostic for pericarditis; all of the following findings can be seen in patients with cardiac ischemia, underlining the importance of approaching pericarditis as a diagnosis of exclusion.
- Widespread/diffuse PR depression and/or ST elevation
- J-point in pericarditis is usually sharper compared to a more blurred J point in MI
- Additional Resources:
- [TW] For an excellent discussion and diagrams of the J point please see the article, J Point, Life In The Fast Lane, Chris Nickson and Mike Cadogan,
- [TW] For an outstanding review of the ST segment, please see the article, The ST Segment, Life In The Fast Lane, Ed Burns and Robert Buttner, Mar 16, 2022
- ST elevations are more commonly convex shaped in STEMI, while concave upwards ST elevations are more typical of pericarditis
- If ST elevation or PR depression is present, there is typically a preservation of the normal upright T-waves in pericarditis (note however, that stage 3 is defined by T-wave inversions)
- ST elevation is rarely > 5mm in pericarditis
- ST depressions in V1 and aVR favor pericarditis
- aVL ST segment is typically elevated in pericarditis while aVL ST segment depression is highly specific for inferior MI
- Comparison of ST elevation in leads II and III may help differentiate STEMI from pericarditis
- ST elevation II > ST elevation III favors pericarditis
- ST elevation III > ST eleveation II is highly suspicious for inferior STEMI
- Spodick’s sign is seen in approximately 80% of patients with acute pericarditis (and in 29% of patients with all stages of pericarditis) and 5% of STEMIs; it is characterized by down-sloping from the T wave to the QRS segments with the terminal PR segment depressed; this is best seen in lead II and the lateral precordial leads.
ECG findings of pericardial effusion that may be associated with pericarditis:
- Low voltages (also seen in COPD, and patients with obesity)
- Electrical alternans
Pitfall: There are no ECG findings that are 100% sensitive for specific to differentiate pericarditis from MI underlining the importance of approaching pericarditis as a diagnosis of exclusion
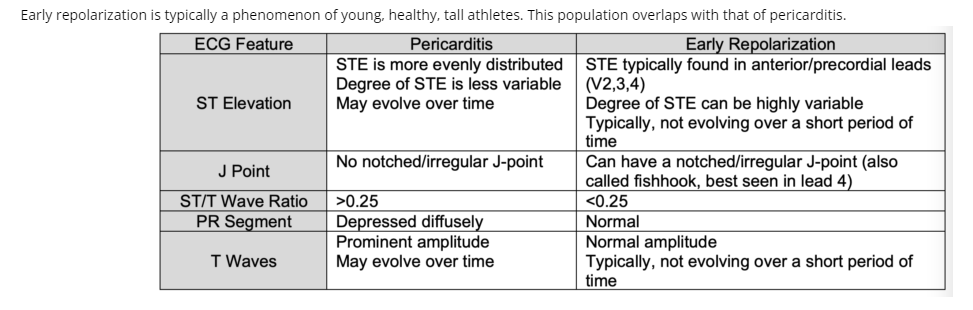
ECG findings to help differentiate pericarditis from early repolarization
PoCUS and pericarditis
Pericardial effusion found on PoCUS supports the diagnosis of pericarditis (60% of patients with pericarditis) but is not diagnostic.
The presence of a large pericardial effusion can help identify patients with acute pericarditis who are at higher risk for complications. If there are signs of LV dysfunction, consider myopericarditis.
To semi-quantitatively describe the size of a pericardial effusion, measure the echo-free space between the pericardial layers at end-diastole.
- Trivial: fluid is only seen in systole
- Small: <10 mm
- Moderate: 10-20 mm
- Large: 21-25mm
- Very Large: >25mm
The larger the pericardial effusion, the more likely cardiac tamponade is present; however, cardiac tamponade may occur with small-moderate pericardial effusions.
Troponin – the importance of trending troponins in suspected pericarditis
Troponin may be elevated in a number of chest pain presentations including pericarditis, myocarditis, pulmonary embolism and ACS. The troponin elevation in pericarditis typically remains stable over hours whereas the troponin elevation in MI typically increases over hours in the acute phase. Only a proportion of patients with pericarditis bump their troponin, and usually to a smaller degree compared to patients with myopericarditis and myocarditis.
Inflammatory markers – their utility in pericarditis
CRP elevation can be somewhat useful to support a diagnosis of pericarditis (a CRP >3 has a sensitivity of 80% for pericarditis). An elevated CRP also suggests a higher risk of recurrence and may be helpful serially to assess the clinical course. A very high CRP increases the likelihood of myopericarditis.
Cardiac Tamponade – a rare life-threatening complication of pericarditis
Pericardial effusion and cardiac tamponade should be considered in all patients with pericarditis, especially those with a non-viral underlying etiology such as malignancy, TB or severe hypothyroidism.
Pearl: The presence of a large pericardial effusion and/or cardiac tamponade increases the likelihood of a non-viral cause of pericarditis and should trigger a search for a non-viral cause.
Cardiac tamponade is a clinical diagnosis, not an imaging one. While the larger the pericardial effusion, the more likely cardiac tamponade, it is not the size of the effusion alone that matters. Rather, it is the pressure on the right side of the heart that is the keystone of tamponade physiology. Small effusions that collect rapidly can lead to tamponade.
Pitfall: a common pitfall in the diagnosis of cardiac tamponade is ruling out tamponade just because the pericardial effusion is small
Clinical features of cardiac tamponade
5 features occur in the majority of patients with tamponade:
- Dyspnea (sensitivity 87-89%)
- Tachycardia (sensitivity, 77%)
- Pulsus paradoxus (with pericardial effusion) >10mmHg (sensitivity, 82%; LR+ 3.3), <10mm Hg (LR-0.03)
- Elevated JVP (sensitivity, 76%)
- Cardiomegaly on chest radiograph (sensitivity, 89%)
Pearl: When the decision to perform a pericardiocentesis needs to be made rapidly, a quick way to assess for pulsus paradoxus is to simply palpate the radial pulse for an inspiratory fall in BP rather than search for a sphygmomanometer (which are sometimes difficult to locate in the ED) and perform the more time-consuming traditional assessment for pulsus paradoxus
PoCUS findings suggestive of cardiac tamponade – scrutinize the right side of the heart and IVC
- A pericardial effusion >25mm (but smaller pericardial effusions can cause tamponade)
- Diastolic right ventricular collapse (high specificity)
- Systolic right atrial collapse (earliest sign)
- A plethoric inferior vena cava with minimal respiratory variation (high sensitivity)
- Exaggerated respiratory cycle changes in mitral and tricuspid valve in-flow velocities as a surrogate for pulsus paradoxus
Pearl: in patients with suspected cardiac tamponade where the diagnosis is not clear, consider a fluid bolus which may make the right heart PoCUS signs and pulsus paradoxus more obvious as well as increase filling pressure and cardiac output (avoid if severe, pre-existing LV dysfunction)
PoCUS Cases pericardial effusion – technique and pitfalls
5 Minute Sono on pericardial tamponade
If the diagnosis of cardiac tamponade is unclear, consider:
- If the patient is clinically stable, a STAT echocardiogram done by an ultrasound tech
- Placing an arterial line for continuous monitoring for pulsus paradoxus
- Performing a pericardiocentesis which is both diagnostic and therapeutic
Pitfall: a common pitfall in the management of cardiac tamponade is delaying pericardiocentesis until the patient becomes hemodynamically unstable
Best Case Ever 31 on pericardiocentesiswith Andrew Sloas
NEJM emergency pericardiocentesis
Treatment of pericarditis – don’t forget the colchicine!
The main goals of the treatment of pericarditis are
1. To reduce the acute inflammation with NSAIDs and
2. To prevent recurrence, constrictive pericarditis and long term morbidity with colchicine.
Be sure to include colchicine because it has been shown to prevent the most common complication of pericarditis – recurrent pericarditis (as apposed to NSAIDs which have not been shown to alter the natural history of acute pericarditis).
Outpatient management of pericarditis with a presumed idiopathic/viral cause
Start here.