In this post I link to and excerpt from Drs Peter Johns’ and James Quinn’s excellent CMAJ article, Clinical diagnosis of benign paroxysmal positional vertigo and vestibular neuritis [No Abstract] [Full-Text HTML] [Ful-Text PDF]. CMAJ. 2020 Feb 24;192(8):E182-E186.
All that follows is from the above outstanding resource.
KEY POINTS
Assess patients with vertigo for focal neurologic signs and symptoms, sustained substantial headache or neck pain, inability to stand and spontaneous vertical nystagmus.
Perform the Dix–Hallpike test only for patients with episodes of vertigo less than 2 minutes and no nystagmus at rest.
Perform the head impulse, nystagmus and test of skew (HINTS) plus (plus refers to a test of recent hearing loss) examination only for patients with hours or days of constant, ongoing vertigo and nystagmus at rest.
Case 1: benign paroxysmal positional vertigo
At 4:00 am, a 71-year-old man turned over in bed onto his left side and experienced a sudden onset of dizziness, described as if the bed was moving. Although lasting only 10–15 seconds, he became sweaty afterwards without nausea or vomiting. He came to the emergency department an hour later. The intense vertigo resolved if he stayed still, but similar brief episodes recurred several times when he laid supine in the hospital. He did not have a headache, neck pain, decreased hearing, paresthesia in his face or limbs, visual field loss, dysarthria, dysphagia, diplopia or dysphonia.
On physical examination, we found no focal weakness, sensory deficit or dysmetria. In the sitting position, he did not have nystagmus while looking straight ahead (spontaneous nystagmus) or when asked to gaze left and then right (gaze-evoked nystagmus). His gait was normal. Because his vertigo was started by head movements and lasted less than a minute and he had no nystagmus, he was a good candidate for positional testing. The patient’s right-sided Dix–Hallpike test was normal, without vertigo or nystagmus. However, during testing of the left side and after a brief latency of 2 or 3 seconds, he had vertigo and nystagmus that lasted 15 seconds. The nystagmus was mostly rotatory, with the upper poles of his eyes beating toward his downward left ear. It became more vertical upward when his gaze was directed toward his upward right ear. This was consistent with a diagnosis of left posterior canal benign paroxysmal positional vertigo (BPPV), which can be best managed using the Epley maneuver (an author video showing this patient’s Dix–Hallpike test and a demonstration of the Epley maneuver is available at https://youtu.be/kvVnEsGVLUY).
Fifteen minutes after completion of the Epley maneuver, repeat Dix–Hallpike testing of the patient’s left ear found no vertigo or nystagmus. Given his clinical presentation and his favourable response to the Epley maneuver, we discharged the patient home with no medication. A follow-up telephone interview 2 weeks after the patient presented to the emergency department determined that he had not had any further dizzy episodes.
Case 2: vestibular neuritis
A 49-year-old man presented to the emergency department with an ongoing, constant spinning sensation for 12 hours that was accompanied by multiple bouts of vomiting. The vertigo persisted to a substantial degree even when the patient remained still, and it worsened with movements such as going from lying down to upright or rapid head turning. He was able to walk unaided but felt unsteady. It was difficult for him to perform tandem gait. He reported that he did not have headache, neck pain or ear symptoms. He also reported that he did not have face or limb paresthesia, focal weakness, dysarthria, dysphagia, diplopia or dysphonia.
On physical examination, we found no motor weakness or dysmetria. We did not observe any vertical nystagmus. Our differential diagnosis was a posterior circulation stroke versus vestibular neuritis, and to differentiate them, we used a clinical examination known as “HINTS plus” (head impulse, nystagmus and test of skew. The term plus refers to a test of recent hearing loss.)
The HINTS plus examination is a series of 4 bedside tests: the type of nystagmus seen, test of skew, head impulse test and a test of hearing.1 Each component of this examination can point to a peripheral or central cause for vertigo. If all 4 results point to a peripheral cause, the overall HINTS plus examination is deemed “HINTS plus peripheral,” and suggests the patient likely has vestibular neuritis. If any of the results are central, the overall result for HINTS plus is deemed “HINTS plus central,” and further workup for stroke is warranted. Based on a study involving 190 patients who presented for emergency medical care with vertigo and nystagmus, the sensitivity and specificity of the HINTS plus examination for identifying a central cause of vertigo was reported as 99% and 97%, respectively.2 The HINTS plus examination should only be conducted for patients with constant ongoing vertigo and spontaneous or gaze-evoked nystagmus. It should not be conducted for patients with transient, brief episodes of vertigo, such as in Case 1, or in patients who do not have spontaneous or gaze-evoked nystagmus.2
The patient in Case 2 had spontaneous left horizontal and slightly rotational nystagmus toward the left ear. The nystagmus increased in amplitude when he looked left. When he looked right, it decreased in intensity but with the fast component still beating toward the left. This type of nystagmus is typical for right vestibular neuritis.3 It is also called unidirectional nystagmus. Results for the patient’s test of skew showed that he had no vertical skew deviation. The result for his head impulse test was normal when his head was turned rapidly to the left, but there was a distinct catch-up saccade seen when his head was quickly turned to the right (an author video showing how to perform and interpret the HINTS plus examination and findings for the patient in Case 2 is available at https://youtu.be/dy6FsKS0LHY).
The patient was able to detect the sound of fingers rubbing beside both his ears, suggesting there was no gross hearing loss.
Taken together, the clinical findings for this patient were consistent with a diagnosis of vestibular neuritis. We advised that he use dimenhydrinate (an over-the-counter antiemetic medication) for the next 3 days as needed for nausea or vomiting. His vertigo improved substantially over the next 2 days, and he recovered completely in 1 week.
Discussion
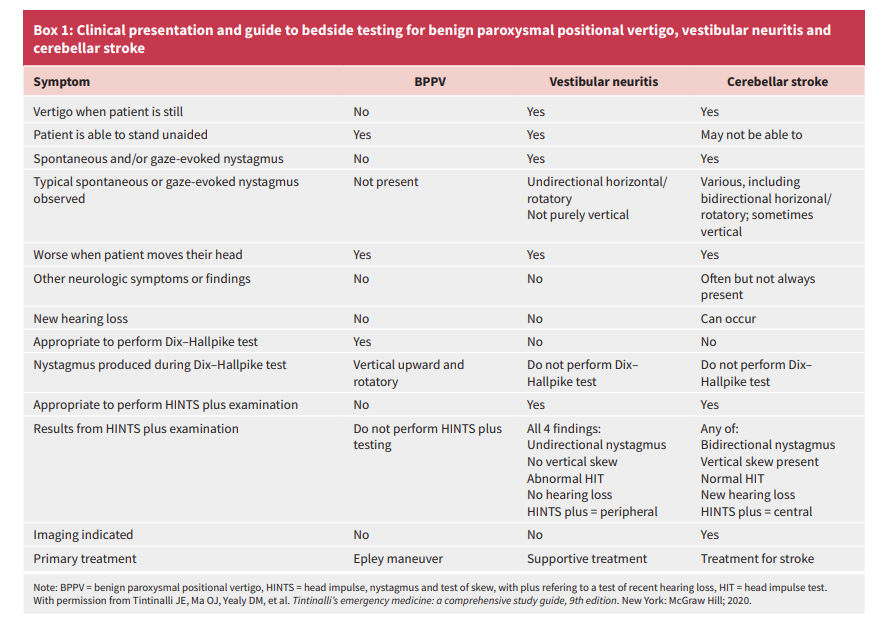
Vertigo is defined as a false or distorted sensation of movement.4 Box 1 presents a comparison of BPPV, vestibular neuritis and cerebellar stroke using important clinical features of each diagnosis, and shows which bedside testing is appropriate, and the characteristic diagnostic findings of bedside testing in these conditions.
Posterior circulation stroke syndromes include transient
ischemic attack (TIA), ischemic and hemorrhagic stroke, and vertebral artery dissection. Hemorrhagic cerebellar stroke and
vertebral artery dissection commonly present with substantial
new and sustained headache or neck pain, respectively.
There are 2 common presentations of peripheral vertigo that
can often be diagnosed using bedside testing.
Benign paroxysmal positional vertigo
Benign paroxysmal positional vertigo is the most common cause
of vertigo.5 It is characterized by brief (typically 20–30 s and
< 2 min) episodes of vertigo started by changes in head position
such as getting in or out of bed, turning over in bed, bending forward or tilting the head backward. If the patient remains still, the intense vertigo sensation ceases.Particles normally found in the utricle find their
way into the semicircular canals and, with head movement,
move within the canals producing vertigo. Benign paroxysmal
positional vertigo is easily treated using particle-repositioning
maneuvers such as the Epley maneuver.5,6A patient with BPPV has no spontaneous or gaze-evoked nystagmus. The Dix–Hallpike test is considered the gold standard for confirming a diagnosis of the most common type of this condition, posterior canal BPPV.5–7 Additional testing is not required in patients with the typical presentation and nystagmus diagnostic of BPPV.6,8
Vestibular neuritis
The most commonly seen cause of substantial continuous dizziness or vertigo and spontaneous nystagmus is vestibular neuritis. Vestibular neuritis and cerebellar stroke can both present with hours to days of ongoing, constant vertigo, spontaneous or gazeevoked nystagmus, nausea or vomiting and difficulty walking. Head movement will briefly exacerbate the patient’s symptoms in both vestibular neuritis and cerebellar stroke. This clinical presentation should be distinguished from the 20–30 second episodes of vertigo started by getting in or out or rolling over in bed, which are typical of BPPV.
Vestibular neuritis is more common than cerebellar stroke
and can be reliably identified using the HINTS plus examination.1Thus, vestibular neuritis, cerebellar stroke and BPPV can
often be diagnosed by combining a clinical history with bedside
testing.5 By ruling in a benign cause of vertigo such as BPPV or
vestibular neuritis, dangerous causes of vertigo are effectively
ruled out.3 This may decrease the use of diagnostic imaging as well as time spent by the patient being evaluated.The most appropriate bedside testing for a patient will depend
on the patient’s clinical presentation. The HINTS plus examination should only be conducted for patients with ongoing vertigo and spontaneous nystagmus. The Dix–Hallpike test should be conducted only for patients with short episodes of vertigo who do not have spontaneous or gaze-evoked nystagmus.2,4
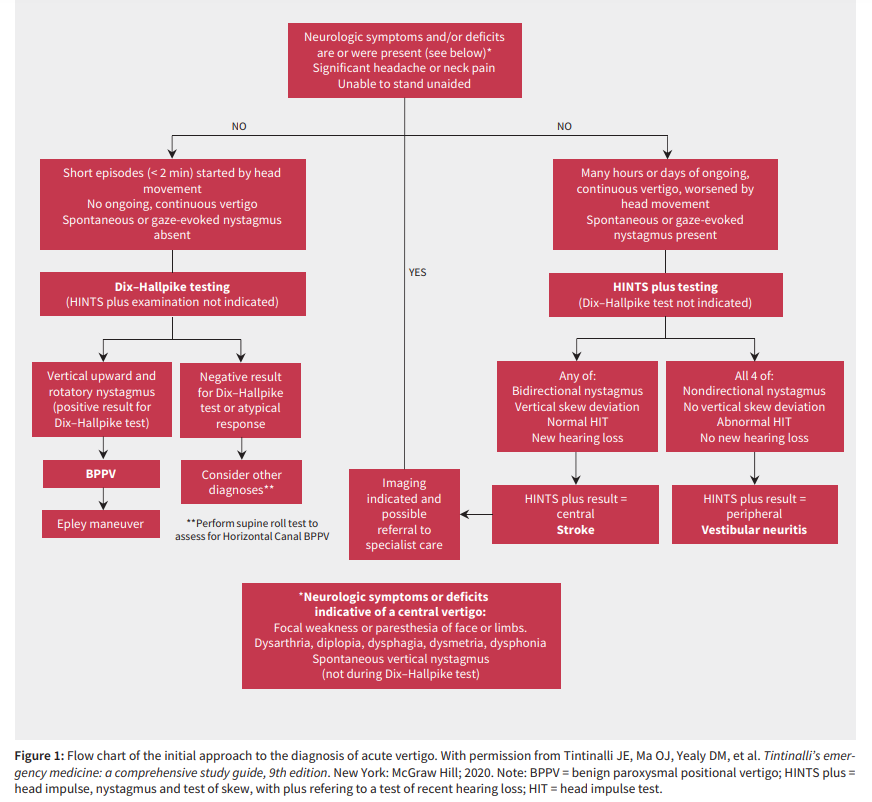
Screening for central features
Using the central portion of Figure 1, clinicians can screen for
neurologic symptoms and deficits from stroke syndromes such
as cerebellar stroke, TIA, cerebellar hemorrhage and vertebral
artery dissection. If a patient screens positive for any of these
findings, they should undergo neuroimaging and referral to specialist care.If a patient screens negative for central features, clinicians
should perform additional bedside testing based on the left or
right arm of the flow chart (Figure 1).Short episodes of vertigo started by head movement
and no spontaneous nystagmusStart here.
Conclusion
With a typical clinical presentation, patients with BPPV can be
diagnosed when the characteristic nystagmus on positional testing is seen. Patients with vestibular neuritis can be differentiated from those with cerebellar stroke with the HINTS plus examination. By reliably diagnosing patients with vertigo using history, physical and appropriately targeted bedside examination techniques, patients can often avoid unnecessary imaging