
In this post, I link to and excerpt from Core IM‘s outstanding podcast and show notes “5 Pearls on Dual Antiplatelet Therapy (DAPT)“.
All that follows is from the episode show notes.

Show Notes
Pearl 1: Indications
Antithrombotic therapy overview
- Antiplatelets (COX1 inhibitor, P2Y12 inhibitor)
- Use in high-velocity flow states
- Myocardial Infarction, Cerebrovascular Accident, Peripheral Arterial Disease, etc.
- Anticoagulants
- Use in low-velocity flow states
- Deep Vein Thrombosis, Pulmonary Embolism, stroke prophylaxis in Atrial Fibrillation, etc.
- Mechanical heart valves
- Use Warfarin (Vitamin K antagonist)
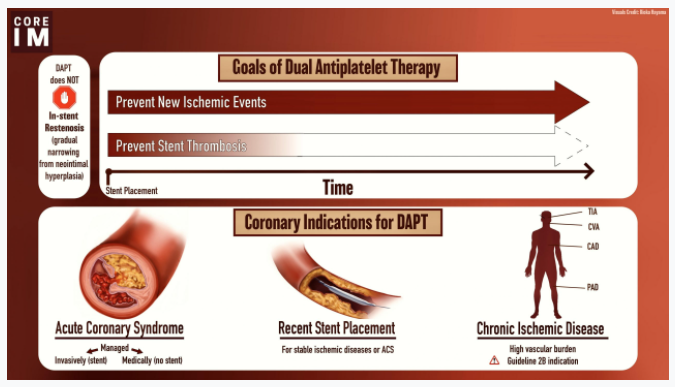
- DAPT indications
- Post-ACS event
- All of these patients should be thought of as a more thrombotic phenotype
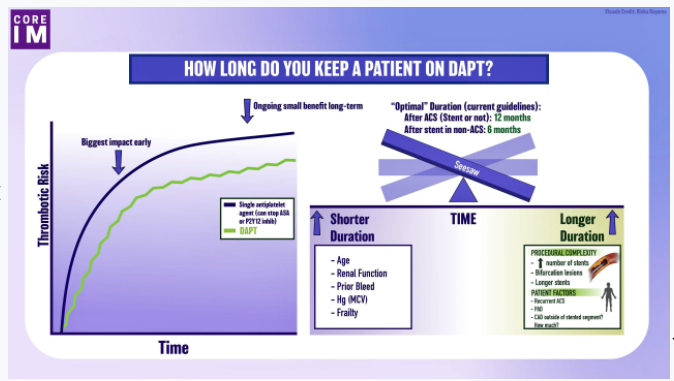
- Therefore, we favor 12 months of DAPT regardless of whether a stent was placed or not
- CURE Trial in 2001 compared Aspirin monotherapy to Aspirin + Clopidogrel for 3-12 months after PCI with a mean duration of 9 months
- Absolute risk reduction of 2.1% for primary composite outcome of cardiovascular death, nonfatal MI, and stroke
- Increased absolute risk of major bleeding by 1%, but did not increase life threatening bleeding
- Stable Ischemic heart disease (SIHD)
- In other words, non-ACS setting
- Can think of these patients as a less thrombotic phenotype
- Consider DAPT if a stent is placed to achieve two primary goals:
- Short term goal
- Reduce risk of stent thrombosis
- Life threatening event which occurs while stent is in process of endothelialization
- Classification and criteria for stent thrombosis
- Important note: Does NOT mitigate risk of in-stent restenosis (which is a more chronic process due to endothelial overgrowth and is not influenced by DAPT)
- Long term goal
- Reduce risk of de novo ischemic events
- Severe diffuse atherosclerosis
- In addition to CAD, antiplatelet agents also have benefit in PAD and cerebrovascular disease
- Phenotypically high-risk group
- May see DAPT in these patients, especially if comorbid CAD
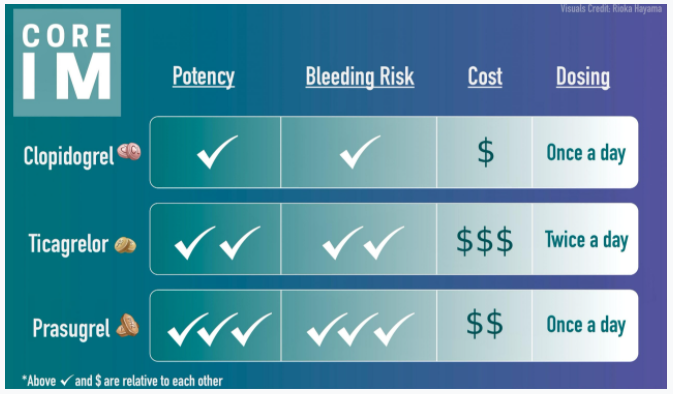
Pearl 2: Medications



