In addition to the links below, please see the CDC web page, Overview of Testing for SARS-CoV-2, the virus that causes COVID-19
Updated Jan. 21, 2022
In addition to the links below, please see the CDC web page, Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Providers.
Updated Oct. 14, 2021
On This Page
______________________________________________________________
Today, I reviewed and link to NIH COVID-19 Guidelines Management.
Clinical Management Summary
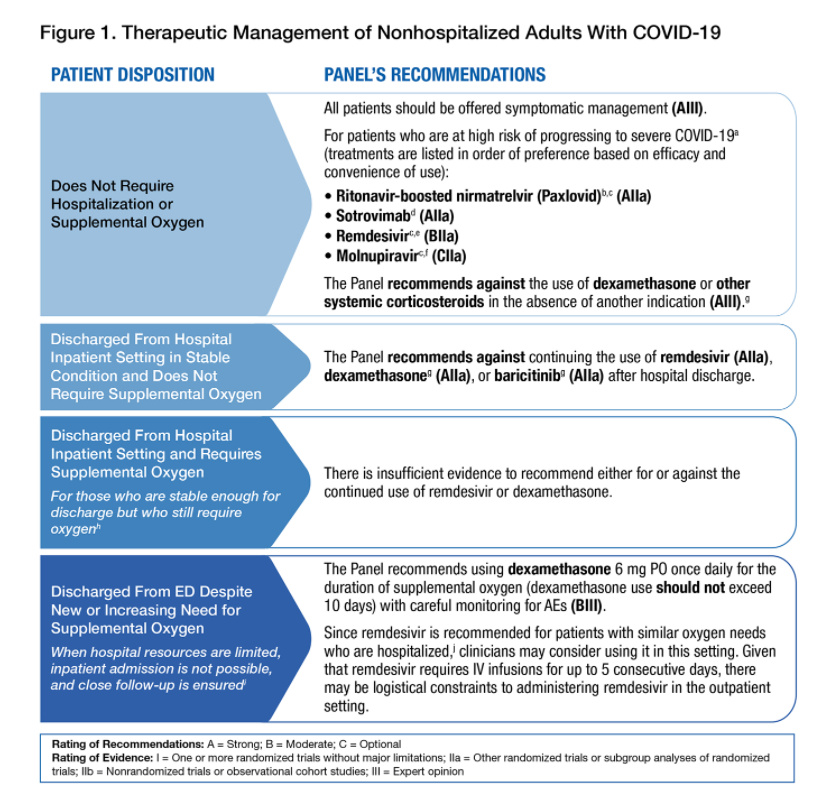
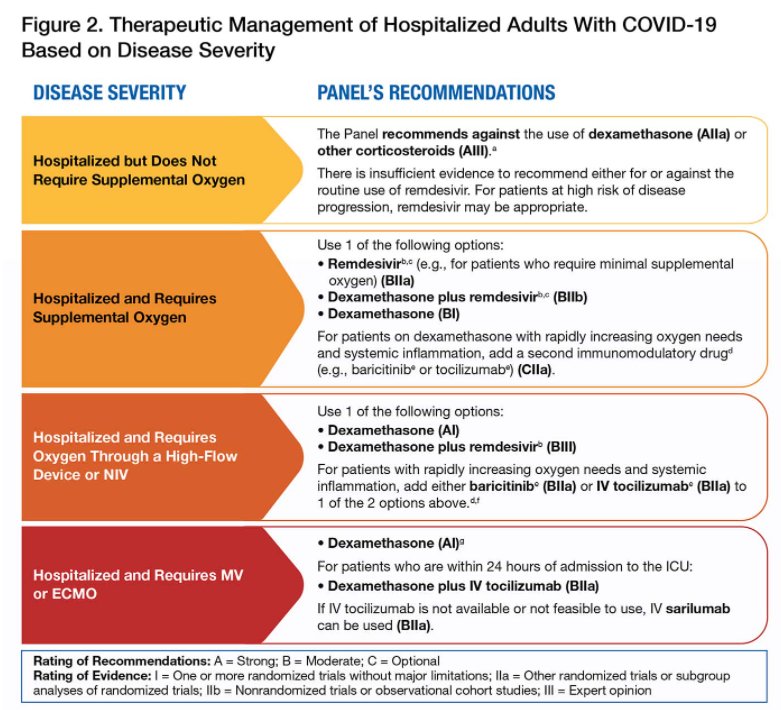
Last Updated: February 1, 2022The clinical spectrum of SARS-CoV-2 infection includes asymptomatic or presymptomatic infection and mild, moderate, severe, and critical illness. Figure 1 provides guidance for clinicians on the therapeutic management of nonhospitalized adult patients. This includes patients who do not require hospitalization or supplemental oxygen and those who have been discharged from an emergency department or a hospital. Figure 2 provides guidance on the therapeutic management of hospitalized adult patients according to their disease severity and oxygen requirements.
For a list of risk factors, see the CDC webpage Underlying Medical Conditions Associated With Higher Risk for Severe COVID-19 and the Patient Prioritization for Treatment section below.
b Ritonavir-boosted nirmatrelvir has significant drug-drug interactions. Clinicians should carefully review a patient’s concomitant medications and evaluate potential drug-drug interactions.
c If a patient requires hospitalization after starting treatment, the full treatment course can be completed at the health care provider’s discretion.
d The B.1.1.529 (Omicron) VOC is currently the dominant SARS-CoV-2 variant in the United States. Sotrovimab is the only anti-SARS-CoV-2 mAb that is active against the Omicron VOC.
e Administration of remdesivir requires 3 consecutive days of IV infusion.
f Molnupiravir has a lower efficacy than the other treatment options. Therefore, it should be used ONLY when the other options are not available or feasible.
g There is currently a lack of safety and efficacy data on the use of these agents in outpatients with COVID-19; using systemic glucocorticoids in this setting may cause harm.
h These individuals should receive oximetry monitoring and close follow-up through telehealth, visiting nurse services, or in-person visits.
i Provide an advanced level of home care, including supplemental oxygen (whether patients are receiving oxygen for the first time or are increasing their baseline oxygen requirements), pulse oximetry, laboratory monitoring, and close follow-up through visiting nurse services, telehealth, or in-person visits.
j See Therapeutic Management of Hospitalized Adults With COVID-19.Key: AE = adverse events; CDC = Centers for Disease Control and Prevention; ED = emergency department; IV = intravenous; mAb = monoclonal antibody; the Panel = the COVID-19 Treatment Guidelines Panel; PO = orally; VOC = variant of concern
General Management of Nonhospitalized Patients With Acute COVID-19
Last Updated: December 16, 2021
Summary Recommendations
- Management of nonhospitalized patients with acute COVID-19 should include providing supportive care, considering the use of COVID-19-specific therapy for patients who have a high risk for disease progression, taking steps to reduce the risk of SARS-CoV-2 transmission (including isolating the patient), and advising patients on when to contact a health care provider and seek an in-person evaluation (AIII).
- When possible, patients with symptoms of COVID-19 should be triaged via telehealth visits to determine whether they require COVID-19-specific therapy and in-person care (AIII).
- Patients with dyspnea should be referred for an in-person evaluation by a health care provider and should be followed closely during the initial days after the onset of dyspnea to assess for worsening respiratory status (AIII).
- Management plans should be based on a patient’s vital signs, physical exam findings, risk factors for progression to severe illness, and the availability of health care resources (AIII).
- See Therapeutic Management of Nonhospitalized Adults With COVID-19 for specific recommendations on using pharmacologic therapy in nonhospitalized patients.
Rating of Recommendations: A = Strong; B = Moderate; C = Optional
Rating of Evidence: I = One or more randomized trials without major limitations; IIa = Other randomized trials or subgroup analyses of randomized trials; IIb = Nonrandomized trials or observational cohort studies; III = Expert opinion
Therapeutic Management of Nonhospitalized Adults With COVID-19
Last Updated: February 1, 2022Several therapeutic options are now available for the treatment of nonhospitalized adults with mild to moderate COVID-19 who are at high risk of disease progression. A number of factors may affect the selection of the best treatment option for a specific patient. These factors include the clinical efficacy and availability of the treatment option, the feasibility of administering parenteral medications (i.e., sotrovimab or remdesivir), the potential for significant drug-drug interactions (e.g., those associated with the use of ritonavir-boosted nirmatrelvir [Paxlovid]), and the regional prevalence of variants of concern (VOC).
See Figure 1 above.
Patient Prioritization for Treatment
During surges in cases of SARS-CoV-2 infection, logistical or supply constraints may make it impossible to offer available therapeutics to all the nonhospitalized patients who are eligible to receive them. In these situations, the Panel recommends prioritizing the treatment of patients who are at the highest risk of clinical progression.
In Table A, the Panel has prioritized the risk groups for anti-SARS-CoV-2 therapy based on 4 key elements: age, vaccination status, immune status, and the presence of risk factors for clinical progression. The groups are listed in descending order of priority. For a list of risk factors, see the Centers for Disease Control and Prevention (CDC) website Underlying Medical Conditions Associated With Higher Risk for Severe COVID-19.
Table A. Patient Risk Groups for Prioritizing the Use of Anti-SARS-CoV-2 Therapy
Tier Risk Group 1
- Immunocompromised individuals who are not expected to mount an adequate immune response to COVID-19 vaccination or SARS-CoV-2 infection due to their underlying conditions, regardless of their vaccine status (see Immunocompromising Conditions below); or
- Unvaccinated individuals who are at the highest risk of severe disease (anyone aged ≥75 years or anyone aged ≥65 years with additional risk factors)
2
- Unvaccinated individuals who are at risk of severe disease and who are not included in Tier 1 (anyone aged ≥65 years or anyone aged <65 years with clinical risk factors)
3
- Vaccinated individuals who are at high risk of severe disease (anyone aged ≥75 years or anyone aged ≥65 years with clinical risk factors)
- Vaccinated individuals who have not received a COVID-19 vaccine booster dose are likely to be at higher risk for severe disease; patients who have not received a booster dose and who are within this tier should be prioritized for treatment.
4
- Vaccinated individuals who are at risk of severe disease (anyone aged ≥65 years or anyone aged <65 with clinical risk factors)
- Vaccinated individuals who have not received a COVID-19 vaccine booster dose are likely to be at higher risk for severe disease; patients who have not received a booster dose and who are within this tier should be prioritized for treatment.
Immunocompromising Conditions
The CDC website COVID-19 Vaccines for Moderately or Severely Immunocompromised People provides a list of moderate and severe immunocompromising conditions.
If these anti-SARS-CoV-2 agents cannot be provided to all moderately to severely immunocompromised individuals because of logistical constraints or supply limitations, the Panel suggests prioritizing their use for those who are least likely to mount an adequate response to COVID-19 vaccination or SARS-CoV-2 infection and who are at risk for severe outcomes. This includes:
- Patients who are within 1 year of receiving B cell-depleting therapies (e.g., rituximab, ocrelizumab, ofatumumab, alemtuzumab)
- Patients who are receiving Bruton tyrosine kinase inhibitors
- Chimeric antigen receptor T cell recipients
- Post-hematopoietic cell transplant recipients who have chronic graft versus host disease or who are taking immunosuppressive medications for another indication
- Patients with hematologic malignancies who are on active therapy
- Lung transplant recipients
- Patients who are within 1 year of receiving a solid organ transplant (other than a lung transplant)
- Solid organ transplant recipients with recent treatment for acute rejection with T cell- or B cell-depleting agents
- Patients with severe combined immunodeficiencies
- Patients with untreated HIV who have a CD4 T lymphocyte cell count <50 cells/mm3
If supplies are extremely limited, the Panel suggests prioritizing those who are more severely immunocompromised (based on the list above) and who have additional risk factors for severe disease.
Table B. Dosing Regimens for the Drugs Recommended for High-Risk, Nonhospitalized Adults With Mild to Moderate COVID-19, Listed in Order of Preference Based on Efficacy and Convenience of Use
Drug Name Dosing Regimen Time From Symptom Onseta Ritonavir-Boosted Nirmatrelvir (Paxlovid) eGFR ≥60 mL/min:
- Nirmatrelvir 300 mg with RTV 100 mg PO twice daily for 5 days
eGFR ≥30 to <60 mL/min:
- Nirmatrelvir 150 mg with RTV 100 mg PO twice daily
eGFR <30 mL/min:
- Not recommended
Severe Hepatic Impairment (Child-Pugh Class C):
- Not recommended
≤5 days Sotrovimab SOT 500 mg as a single IV infusion ≤10 days Remdesivir RDV 200 mg IV on Day 1, followed by RDV 100 mg IV once daily on Days 2 and 3b,c ≤7 days Molnupiravir Molnupiravir 800 mg PO twice daily for 5 days ≤5 days a Per EUA criteria or clinical trial entry criteria. b An eGFR <30 mL/min at screening or <90 days before screening was considered an exclusion criterion in the outpatient RDV study PINETREE, but only if a participant’s weight was <48 kg. See the Remdesivir section for a discussion of RDV use in patients with renal impairment.
c If RDV is administered to patients who have a new or increasing need for supplemental oxygen but who are discharged from the ED because hospital resources are limited and inpatient admission is not possible, the total duration of therapy is ≤5 days.
Key: ED = emergency department; eGFR = estimated glomerular filtration rate; EUA = Emergency Use Authorization; IV = intravenous; PO = orally; RDV = remdesivir; RTV = ritonavir; SOT = sotrovimab
Symptom Management
Symptomatic treatment includes using over-the-counter antipyretics, analgesics, or antitussives for fever, headache, myalgias, and cough. Patients with dyspnea may benefit from resting in the prone position rather than the supine position.1 Health care providers should consider educating patients about breathing exercises, as severe breathlessness may cause anxiety.2 Patients should be advised to drink fluids regularly to avoid dehydration. Rest is recommended as needed during the acute phase of COVID-19, and ambulation and other forms of activity should be increased according to the patient’s tolerance. Patients should be educated about the variability in time to symptom resolution and complete recovery.
Rationale for the Use of Specific Agents Listed in Figure 1
The Panel’s recommendations and preferences for the therapeutics that are used to treat nonhospitalized patients with COVID-19 are based on the results of clinical trials for ritonavir-boosted nirmatrelvir, remdesivir, and molnupiravir, and on the results of clinical trials and laboratory assessments of the activity of the anti-SARS-CoV-2 monoclonal antibody (mAb) products that are currently available through Emergency Use Authorizations (EUAs) from the Food and Drug Administration (FDA) for the treatment of COVID-19. These therapies are recommended for patients with mild to moderate COVID-19 who are at high risk of progressing to severe disease.
It should be noted that a number of factors affect the selection of the best treatment option for a specific patient. These factors include the clinical efficacy and the availability of the treatment option, the feasibility of administering parenteral medications (i.e., sotrovimab, remdesivir), and the potential for significant drug-drug interactions (i.e., the interactions associated with using ritonavir-boosted nirmatrelvir).
The Panel favors the use of ritonavir-boosted nirmatrelvir in most high-risk, nonhospitalized patients with mild to moderate COVID-19. If ritonavir-boosted nirmatrelvir is not available or cannot be used because of drug interactions, the Panel recommends using the anti-SARS-CoV-2 mAb sotrovimab as the second option. If sotrovimab is not available, then the Panel recommends using remdesivir. Molnupiravir should ONLY be used when the other 3 options are either not available or cannot be used.
There are currently no clinical trial data that directly compare the clinical efficacy of these 4 therapies, and there are no data on the use of combinations of antiviral agents and/or anti-SARS-CoV-2 mAbs for the treatment of COVID-19. The rationale for each of the Panel’s recommendations is discussed below.
Please see the webpage for details of the above recomendations.
Concomitant Medication Management
In general, a patient’s usual medication and/or supplement regimen should be continued after the diagnosis of COVID-19 (see Considerations for Using Concomitant Medications in Patients With COVID-19). Angiotensin-converting enzyme inhibitors, statin therapy, nonsteroidal anti-inflammatory drugs, and oral, inhaled, and intranasal corticosteroids that are prescribed for comorbid conditions should be continued as directed (AIII). Patients should be advised to avoid the use of nebulized medications in the presence of others to avoid potential aerosolization of SARS-CoV-2.19 In patients with HIV, antiretroviral therapy should not be switched or adjusted for the purpose of preventing or treating SARS-CoV-2 infection (AIII). For more information, see Special Considerations in People With HIV.
When a patient is receiving an immunomodulating medication, the prescribing clinician should be consulted about the risks and benefits that are associated with a temporary dose reduction or discontinuation; these risks and benefits will depend on the medication’s indication and the severity of the underlying condition.
Patients who use a continuous positive airway pressure (CPAP) device or a bilevel positive airway pressure (BiPAP) device to manage obstructive sleep apnea may continue to use their machine. As with nebulizers, patients should be advised to use the device only when they are isolated from others.
Therapeutic Management of Hospitalized Adults With COVID19 Last Updated: December 16, 2021
In addition to pulmonary disease, critically ill patients with COVID-19 may experience cardiac, hepatic, renal, and central nervous system disease.