Today, I review, link to, and post the notes on “Sarah Reid on an approach to infant vomiting” from Emergency Medicine Cases Quick Hits #52.* This segment of the podcast runs from 1:08 – 10:43.
*Helman, A. Reid, S. Long, B. Morgenstern, J. Shenvi, C. Hine, J. Billin, A. EM Quick Hits 52 – Infant Vomiting, Orbital Cellulitis, Prehospital TXA in Trauma, Prevention and Treatment of Delirium, Procedural Skills Decay, Altitude Sickness. Emergency Medicine Cases. October, 2023. https://emergencymedicinecases.com/em-quick-hits-october-2023/. Accessed October 20, 2023.
All that follows is from the show notes of Dr. Reid’s lecture.
Approach to infant vomiting
Infant vomiting DDx
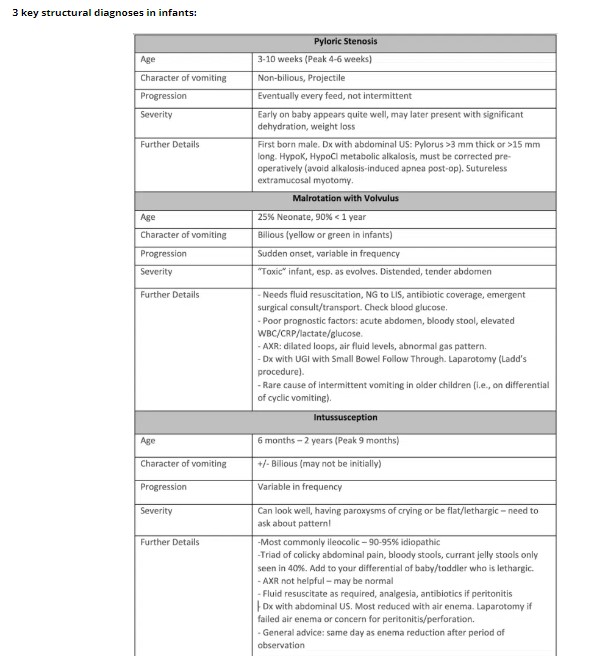
- Structural/Surgical: pyloric stenosis, malrotation with volvulus, intussusception, incarcerated hernia, ovarian/testicular torsion, bowel stenosis/atresia, Hirschprung’s disease
- Infectious: UTI, otitis media, pharyngitis, pneumonia, CNS (see below), gastroenteritis, URTI, pertussis
- GI: GER/GERD, overfeeding, Cow’s Milk Protein Allergy (CMPA), Food Protein-Induced Enterocolitis Syndrome (FPIES)
- CNS: mass, bleed, hydrocephalus, meningitis, encephalitis, brain abscess, congenital lesion, trauma, child maltreatment
- Metabolic/Endocrine: inborn error of metabolism, adrenal insufficiency, DKA (very rare in infants)
General approach to infant vomiting
- Is the baby sick or not?
- Is there fever or not? Septic workup or not?
- Characteristics and pattern of vomiting.
- Is this bilious/yellow/green/bloody?
- Is there a progression of vomiting (intermittent or every feed). Pyloric stenosis is classic for vomiting with every feed.
- Assess for behaviour sometimes linked with intussusception.
- Crying episodes, hard to console, seem in pain, drawing up their knees. Interspersed with periods of being quite well or the baby being pale lethargic. Can be (intussusception, severe illness, CNS process)
Physical exam pearls for pediatric vomiting
A head to toe exam is essential, including:
- Assess fontanelles for dehydration vs raised ICP
- Look in the diaper for an inguinal hernia, undescended testes, testicular torsion
The child with vomiting who is otherwise well
The normal baby with normal vitals, no blood or bile in their vomiting, vomiting intermittently, tolerating feeds in between and maintaining their hydration with an otherwise normal physical is usually an early viral illness versus GERD.
Checklist for safe discharge in pediatric vomiting
- Normal vitals
- No bile/blood
- Intermittent/few episodes of vomiting, tolerating feeds/oral rehydration in between.
- Well hydrated, able to maintain hydration.
- Normal full exam
Discharge instructions and disposition for pediatric vomiting
PCP follow-up in a few days, return to ED if persistent vomiting over a few feeds, any yellow/green/blood in vomit, less than 4 wet diapers in 24 hours, very sleepy/hard to wake, irritable/crying/pain/episodes of inconsolability, fever x 2-3 days