Guideline-directed medical therapy (GDMT) for heart failure (HF) with reduced ejection fraction (HFrEF) now includes 4 medication classes that include sodium-glucose cotransporter-2 inhibitors (SGLT2i).
2.
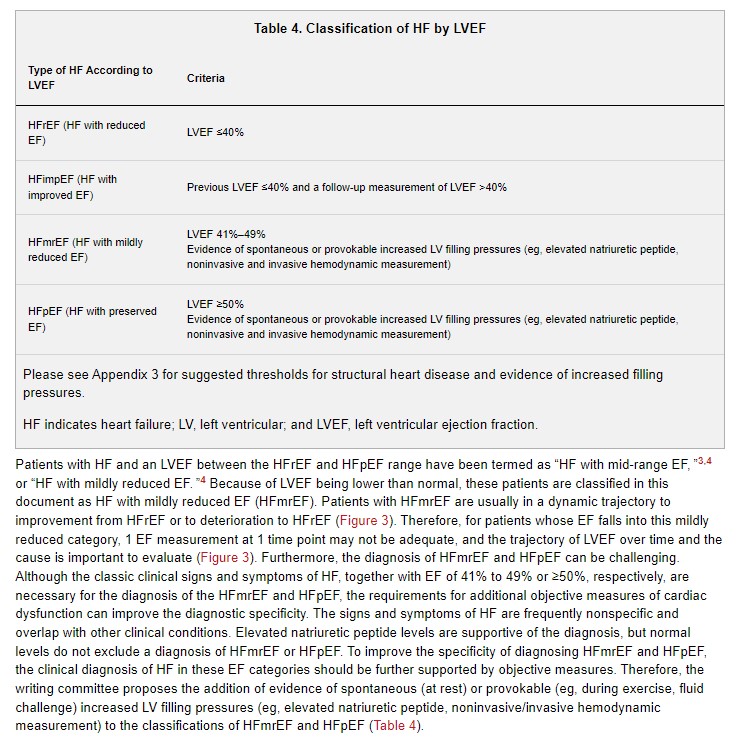
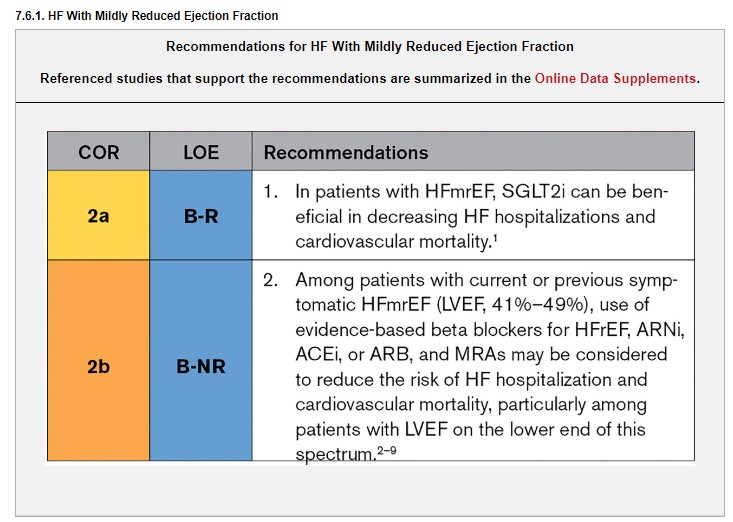
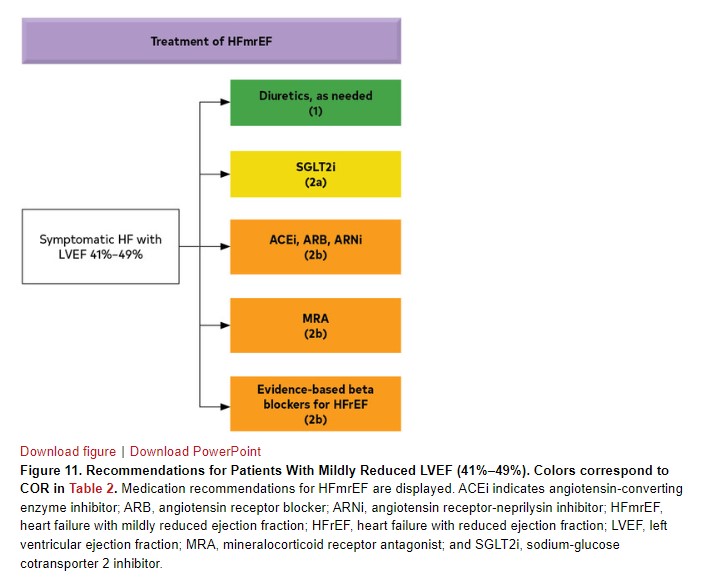
SGLT2i have a Class of Recommendation 2a in HF with mildly reduced ejection fraction (HFmrEF). Weaker recommendations (Class of Recommendation 2b) are made for ARNi, ACEi, ARB, MRA, and beta blockers in this population.
3.
New recommendations for HFpEF are made for SGLT2i (Class of Recommendation 2a), MRAs (Class of Recommendation 2b), and ARNi (Class of Recommendation 2b). Several prior recommendations have been renewed including treatment of hypertension (Class of Recommendation 1), treatment of atrial fibrillation (Class of Recommendation 2a), use of ARBs (Class of Recommendation 2b), and avoidance of routine use of nitrates or phosphodiesterase-5 inhibitors (Class of Recommendation 3: No Benefit).
4.
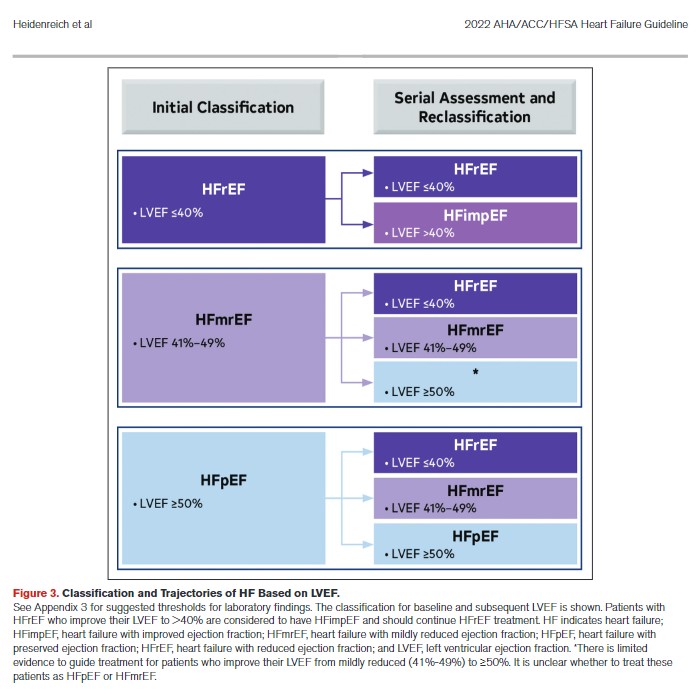
Improved LVEF is used to refer to those patients with previous HFrEF who now have an LVEF >40%. These patients should continue their HFrEF treatment.
5.
Value statements were created for select recommendations where high-quality, cost-effectiveness studies of the intervention have been published.
6.
Amyloid heart disease has new recommendations for treatment including screening for serum and urine monoclonal light chains, bone scintigraphy, genetic sequencing, tetramer stabilizer therapy, and anticoagulation.
7.
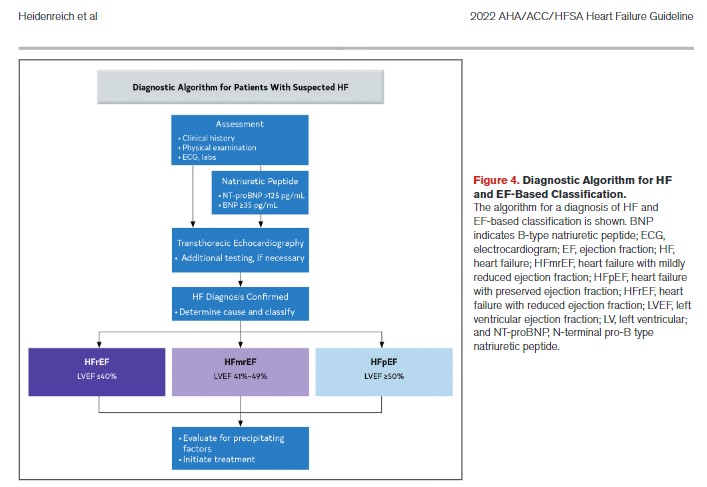
Evidence supporting increased filling pressures is important for the diagnosis of HF if the LVEF is >40%. Evidence for increased filling pressures can be obtained from noninvasive (eg, natriuretic peptide, diastolic function on imaging) or invasive testing (eg, hemodynamic measurement).
8.
Patients with advanced HF who wish to prolong survival should be referred to a team specializing in HF. A HF specialty team reviews HF management, assesses suitability for advanced HF therapies, and uses palliative care including palliative inotropes where consistent with the patient’s goals of care.
9.
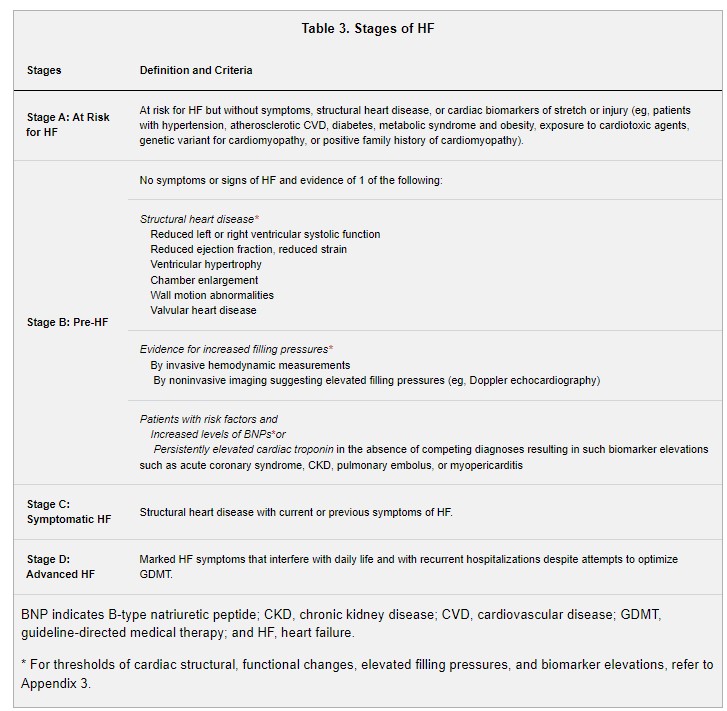
Primary prevention is important for those at risk for HF (stage A) or pre-HF (stage B). Stages of HF were revised to emphasize the new terminologies of “at risk” for HF for stage A and pre-HF for stage B.
10.
Recommendations are provided for select patients with HF and iron deficiency, anemia, hypertension, sleep disorders, type 2 diabetes, atrial fibrillation, coronary artery disease, and malignancy.
2.1. Stages of HF
The ACC/AHA stages of HF (Figure 1, Table 3) emphasize the development and progression of disease,1,2 and advanced stages and progression are associated with reduced survival.3 Therapeutic interventions in each stage aim to modify risk factors (stage A), treat risk and structural heart disease to prevent HF (stage B), and reduce symptoms, morbidity, and mortality (stages C and D). To address the evolving role of biomarkers and structural changes for recognition of patients who are at risk of developing HF, who are potential candidates for targeted treatment strategies for the prevention of HF, and to enhance the understanding and adoption of these classifications, the writing committee proposed the terminologies listed in Table 3 for the stages of HF. For thresholds of cardiac structural, functional changes, elevated filling pressures, and biomarker elevations, refer to Appendix 3.
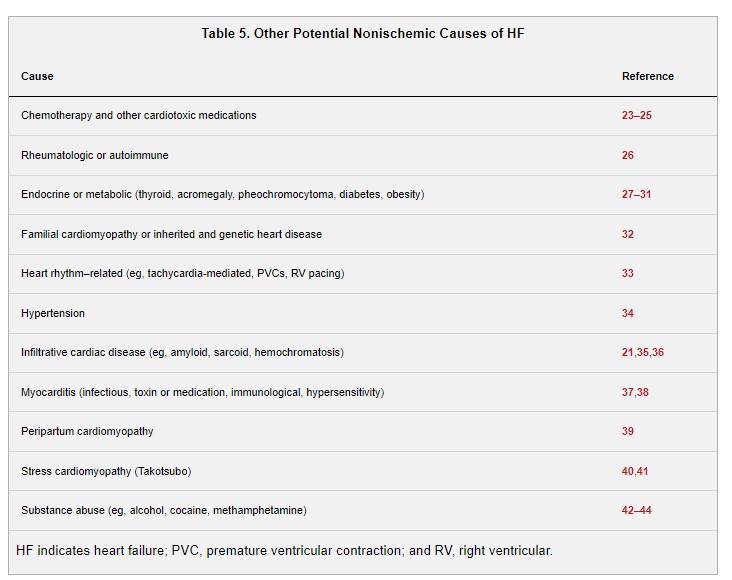
The common causes of HF include ischemic heart disease and myocardial infarction (MI), hypertension, and valvular heart disease (VHD).
4. Initial and Serial Evaluation
Synopsis
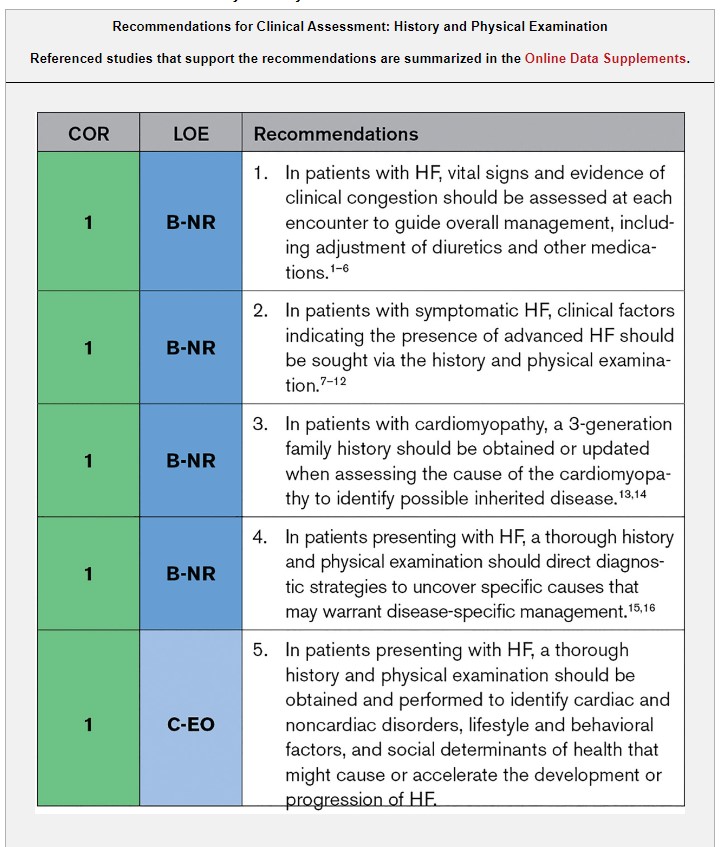
The history and physical examination remain a cornerstone in the assessment of patients with HF. The history and physical examination provide information about the cause of an underlying cardiomyopathy, including the possibility of an inherited cardiomyopathy as ascertained by a family history or a condition requiring disease-specific therapy like amyloid heart disease, as well as reasons why a previously stable patient developed acutely decompensated HF. A critical component of the history and physical examination is to assess for clinical congestion (ie, those signs and symptoms resulting from elevated cardiac filling pressures). Congestion is a target for medication adjustment and is associated with quality of life (QOL) and prognosis. The history and physical examination also allow for the determination of clinical clues that suggest the patient has advanced HF, which may warrant referral to an advanced HF center.
Synopsis
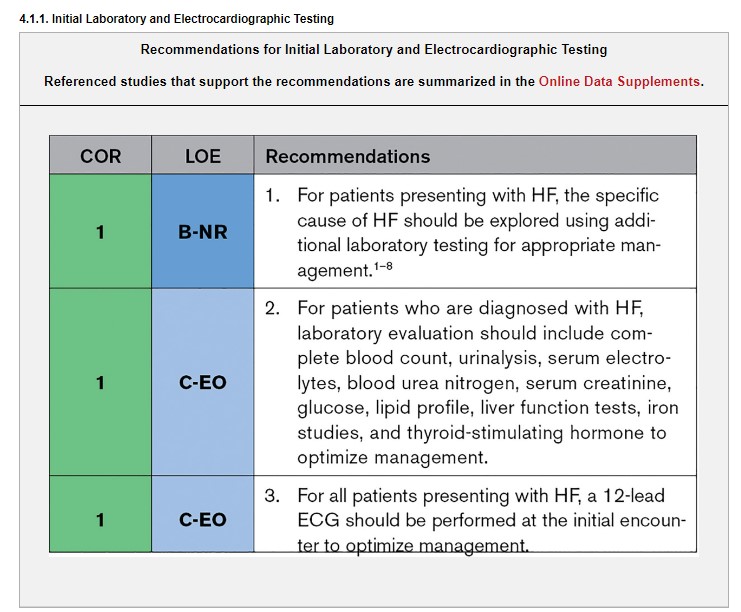
Laboratory evaluation with complete blood count, urinalysis, serum electrolytes (including sodium, potassium, calcium, and magnesium), blood urea nitrogen, serum creatinine, glucose, fasting lipid profile, liver function tests, iron studies (serum iron, ferritin, transferrin saturation), and thyroid-stimulating hormone level and electrocardiography is part of the standard diagnostic evaluation of a patient with HF. In addition to routine assessment, specific diagnostic testing and evaluation is often necessary to identify specific cause and other comorbidities in patients with HF.
Synopsis
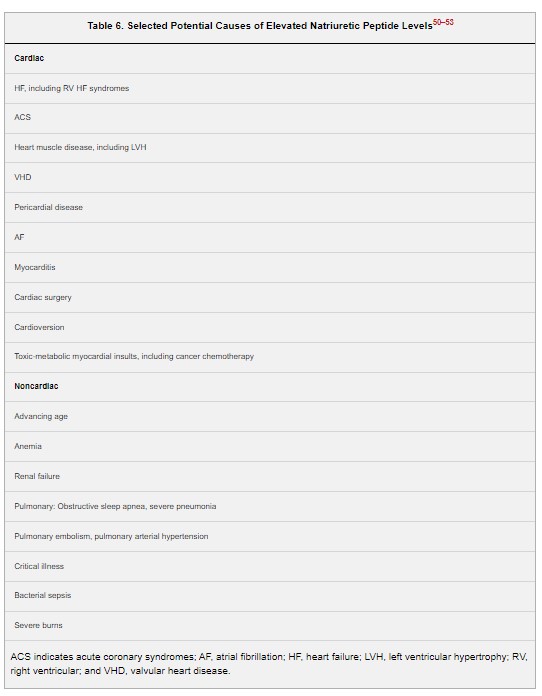
Assays for BNP and NT-proBNP are frequently used to establish the presence and severity of HF. In general, BNP and NT-proBNP levels are similar, and either can be used in patient care settings as long as their respective absolute values and cut-points are not used interchangeably.32–34 Obesity is associated with lower levels of BNP and NT-proBNP thereby reducing their diagnostic sensitivity.35,36 A substantial evidence base supports the use of natriuretic peptide biomarkers for excluding HF as a cause of symptoms in ambulatory and emergency department settings. Although a reduction in BNP and NT-proBNP has been associated with better outcomes, the evidence for treatment guidance using serial BNP or NT-proBNP measurements remains insufficient.37–39 Lastly, a widening array of biomarkers including markers of myocardial injury, inflammation, oxidative stress, vascular dysfunction, and matrix remodeling have been shown to provide incremental prognostic information over natriuretic peptides but remain without evidence of an incremental management benefit.13,40–49
Synopsis
In patients in whom a genetic or inherited cardiomyopathy is suspected, a family history should be performed, including at least 3 generations and ideally diagrammed as a family tree pedigree (see Section 4.1, “Clinical Assessment: History and Physical Examination”). Genetic variants have been implicated in 25% to 40% of patients with DCM with a positive family history but also in 10% to 30% of patients without a recognized family history.3,4 Phenotype and family history are important for identifying patients in whom genetic testing is most likely to yield clinically actionable information (Table 7). Presentation of DCM with conduction disease or ventricular arrhythmias raises concern of sarcoidosis and arrhythmogenic cardiomyopathy, which is of particular concern because of the risk of sudden death in patients and families.5 No controlled studies have shown clinical benefits of genetic testing for cardiomyopathy, but genetic testing contributes to risk stratification and has implications for treatment, currently most often for decisions regarding defibrillators for primary prevention of sudden death5 and regarding exercise limitation for hypertrophic cardiomyopathy and the desmosomal variants. Consultation with a trained counselor before and after genetic testing helps patients to understand and weigh the implications of possible results for their own lives and those of family members, including possible discrimination on the basis of genetic information. Unless shown to be free of the genetic variant(s) implicated in the proband, first-degree relatives of affected probands should undergo periodic screening with echocardiography and electrocardiography.
Synopsis
Cardiac imaging has a key role in the initial evaluation of individuals with suspected HF and, when indicated, in the serial assessment of patients with HF. After a complete history and physical examination, a comprehensive TTE is the most useful initial diagnostic test given the vast amount of diagnostic and prognostic information provided. The determination of LVEF is a fundamental step to classify HF and to guide evidence-based pharmacological and device-based therapy. In certain situations, the echocardiogram is unable to accurately assess cardiac structure and/or function or more information is needed to determine the cause of the cardiac dysfunction. Other imaging modalities, such as CMR, SPECT or radionuclide ventriculography, PET, or cardiac CT or invasive coronary angiography, can provide additional and complementary information to cardiac ultrasound.11 In general, cardiac imaging tests, including repeat tests, are performed only when the results have a meaningful impact on clinical care.
Synopsis
Invasive evaluation of patients with HF may provide important clinical information to determine the cause of HF and treatment options. Routine right heart catheterization does not provide sufficient information to guide treatment decisions.3,4 However, hemodynamic evaluation with right heart catheterization and monitoring in the setting of acute respiratory distress, systemic hypoperfusion including cardiogenic shock, or when hemodynamics are uncertain, may guide treatment decisions. Coronary angiography may be useful in patients who are candidates for revascularization7–9 (see Section 4.4, “Evaluation with Cardiac Imaging,” for recommendations). Endomyocardial biopsy may be advantageous in patients with HF in which a histological diagnosis, such as amyloidosis or myocarditis, may influence treatment decisions.1,2
Synopsis
HF is a chronic condition punctuated by periods of instability. Despite close longitudinal monitoring via in-person visits, event rates remain high, affording a potential role for remote monitoring strategies to improve clinical outcomes. Strategies tested in randomized trials include an implantable PA pressure sensor (CardioMEMS), noninvasive telemonitoring, or monitoring via existing implanted electronic devices (ICDs or CRT-Ds). Results from a single randomized trial,1–3 and subsequent observational studies,8–10 support consideration of an implantable PA sensor in selected patients with HF to reduce the risk of HF hospitalization. In contrast, a recent trial testing a PA pressure sensor did not meet its primary endpoint.4 Results from previous clinical trials do not support the alternative remote monitoring strategies (eg, noninvasive telemonitoring or remote monitoring of physiological parameters such as patient activity, thoracic impedance, heart rate) for this purpose.11–18
Synopsis
Functional impairment and exercise intolerance are common in HF. CPET and the 6-minute walk test are standardized, reliable, and reproducible tests to quantify functional capacity.19–22 The NYHA functional classification can be used to grade the severity of functional limitation based on patient report of symptoms experienced with activity1 and is used to define candidates for certain treatments.
Synopsis
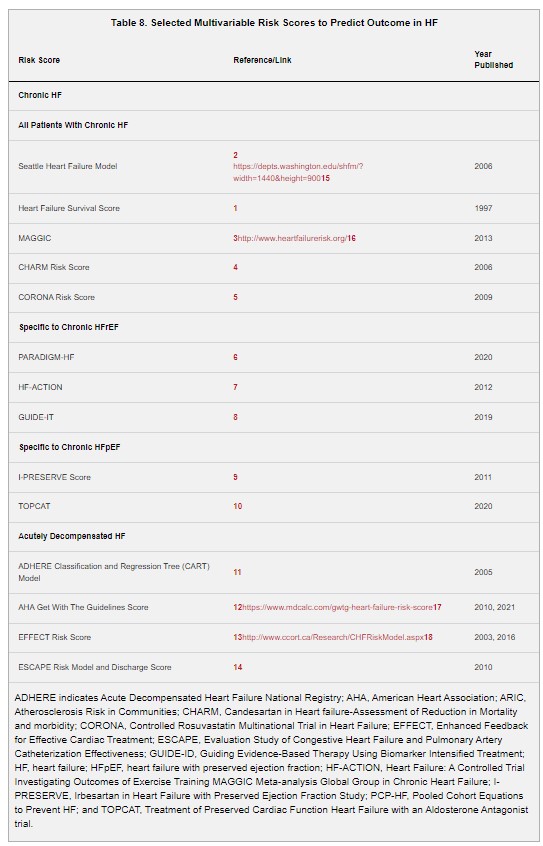
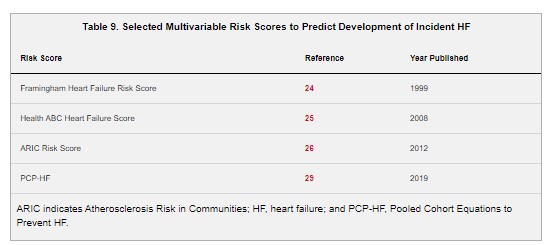
Clinicians should routinely assess a patient’s risk for an adverse outcome to guide discussions on prognosis, goals of care, and treatment decisions. Several predictive models of outcomes of patients with HF have been developed and validated using data from clinical trials, registries, and population-based cohorts. The best performing models have focused on predicting short- and long-term mortality, whereas predictive models for hospitalization or readmission for HF have generally had poor or modest discrimination. Predictive models may also assess the risk of incident HF among the general population and should be considered in the prevention of HF. In the course of standard evaluation, clinicians should routinely assess the patient’s potential for adverse outcome, because accurate risk stratification may help guide therapeutic decision-making, including a more rapid transition to advanced HF therapies. Several methods objectively assess risk (Table 8), including biomarker testing, as well as various multivariable clinical risk scores, and some that include machine learning.1–14 These risk scores are for use in ambulatory, hospitalized patients, and the general population.
Recommendation-Specific Supportive Text
1.
For HF, there are several clinical models to consider that include the spectrum of HF based on EF and clinical setting. For chronic HF, the Seattle Heart Failure Model,2 the Heart Failure Survival score,1 and the MAGGIC score3 have commonly been used to provide estimates of survival. The MAGGIC predictive model may be quite useful given its derivation and validation across multiple clinical trials and cohorts, including more recent studies. For chronic HFrEF, there are additional models that include other clinical variables, including exercise capacity7 and natriuretic peptide levels.8 Likewise, for chronic HFpEF there are more specific predictive models for that population derived from clinical trial data.9,10 In acute HF, several clinical models may be used to predict short-term survival.11–13
5. Stage A (Patients at Risk for HF)
Synopsis
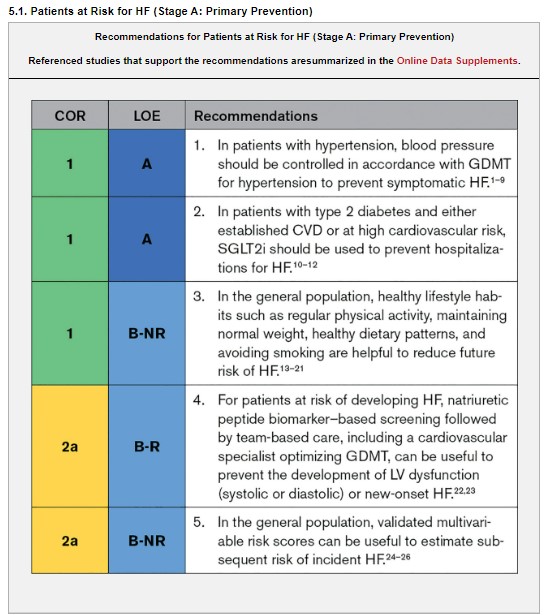
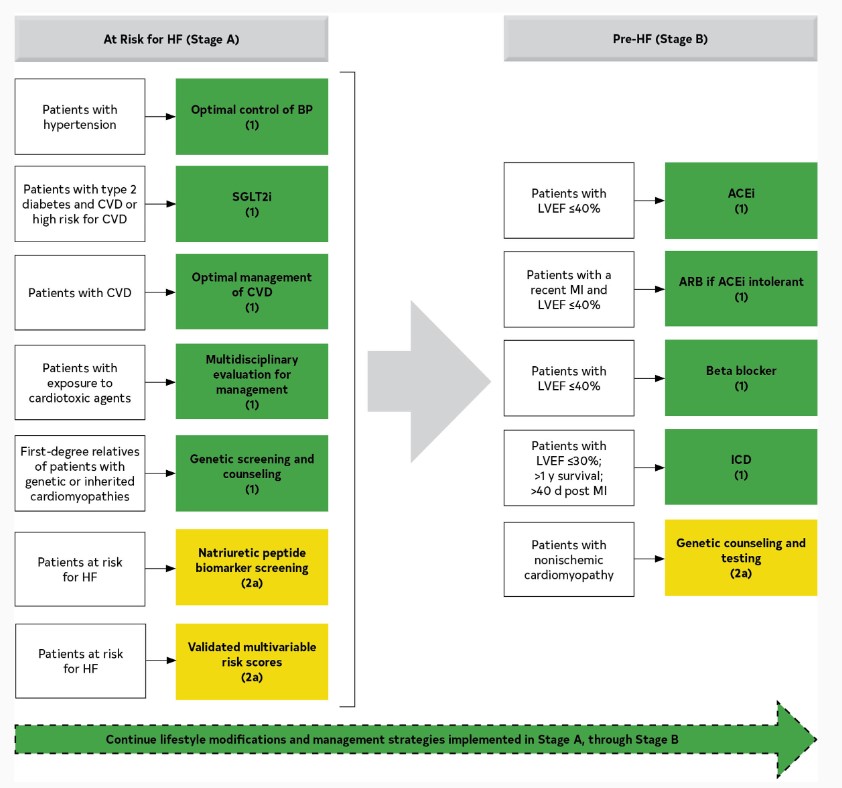
Healthy lifestyle habits such as maintaining regular physical activity; normal weight, blood pressure, and blood glucose levels; healthy dietary patterns, and not smoking reduce primordial risk and have been associated with a lower lifetime risk of developing HF.13–21,27 The AHA/ACC primary prevention guidelines provide recommendations for diet, physical activity, and weight control, all of which have been associated with the risk of HF.28 Blood pressure is an important risk factor for HF, and a treatment goal of <130/80 mm Hg is recommended for those with a CVD risk of ≥10%.29,30 Multiple RCTs have found that patients with diabetes and CVD without HF have improved survival and reduced HF hospitalizations with SGLT2i.31 Patients at risk for HF screened with BNP or NT-proBNP followed by collaborative care, diagnostic evaluation, and treatment in those with elevated levels can reduce combined rates of LV systolic dysfunction, diastolic dysfunction, and HF.22,23 See Figure 5 for COR 1 and 2a for stage A (at risk for HF) and stage B (pre-HF).
Figure 5.Recommendations (Class 1 and 2a) for Patients at Risk of HF (Stage A) and Those With Pre-HF (Stage B). Colors correspond to COR in Table 2. COR 1 and COR 2a for patients at risk for HF (stage A) and those with pre-HF (stage B) are shown. Management strategies implemented in patients at risk for HF (stage A) should be continued though stage B. ACEi indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BP, blood pressure; COR, Class of Recommendation; CVD, cardiovascular disease; HF, heart failure; ICD, implantable cardioverter-defibrillator; LVEF, left ventricular ejection fraction; MI, myocardial infarction; and SGLT2i, sodium glucose cotransporter 2 inhibitor.
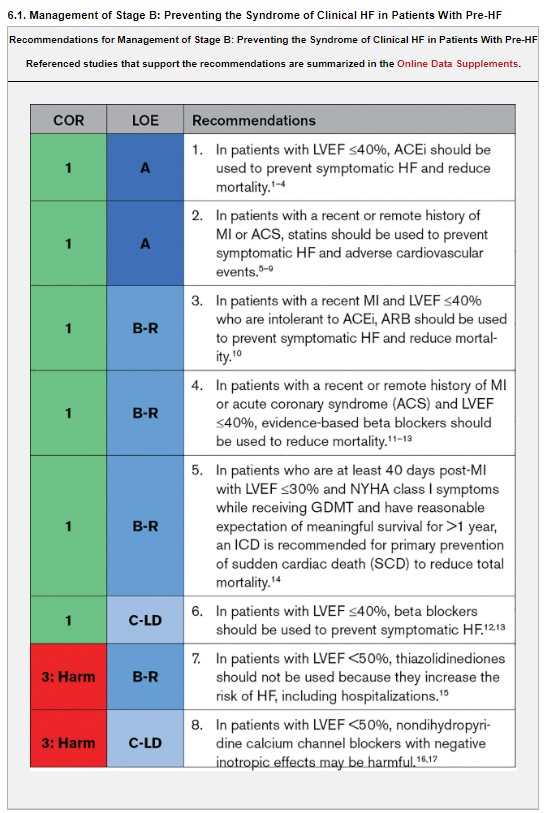
6. Stage B (Patients With Pre-HF)
Synopsis
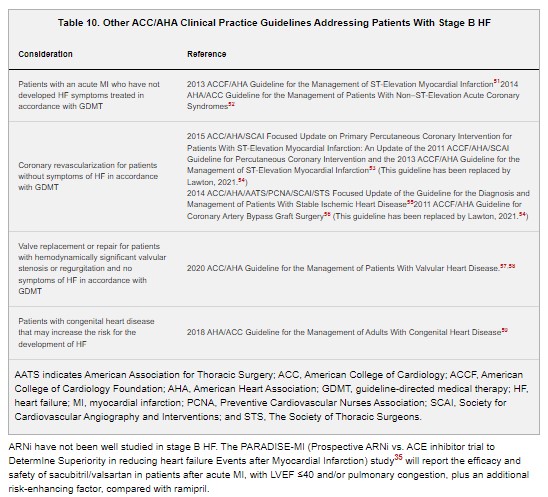
In general, all recommendations for patients with stage A HF also apply to those with stage B HF. Stage B (pre-HF) represents a phase of clinically asymptomatic structural and functional cardiac abnormalities that increases the risk for symptomatic HF.18–21 Identifying individuals with stage B HF provides an opportunity to initiate lifestyle modification and pharmacological therapy that may prevent or delay the transition to symptomatic HF (stage C/D). Several ACC/AHA clinical practice guidelines address appropriate management of patients with stage B HF (Table 10). Although multiple studies highlight the increased HF risk associated with asymptomatic LV systolic19,20,22–26 and diastolic dysfunction identified by noninvasive imaging,19,26–30 beneficial pharmacotherapy for asymptomatic LV systolic dysfunction, such as inhibitors of the renin-angiotensin system and beta blockers, have been predominantly observed in individuals with depressed LVEF (LVEF <35%–40%).1–4,11–13 Studies of specific treatments to alter the onset of HF in the setting of asymptomatic cardiac dysfunction with preserved LVEF (eg, abnormalities of myocardial deformation or diastolic dysfunction) have been limited. Several comorbid conditions, including diabetes, obesity, and hypertension, have been associated with asymptomatic LV dysfunction27,28,30,31 and with progression of asymptomatic LV dysfunction to symptomatic HF.27 Accordingly, these comorbidities are controlled according to current clinical practice guidelines. The benefits of mineralocorticoid receptor antagonists (MRA) after MI have mostly been shown in patients with symptomatic HFrEF.32–34
7. Stage C HF
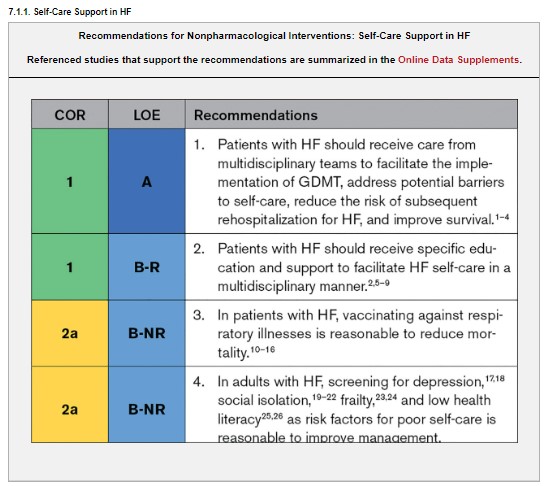
7.1. Nonpharmacological Interventions
Synopsis
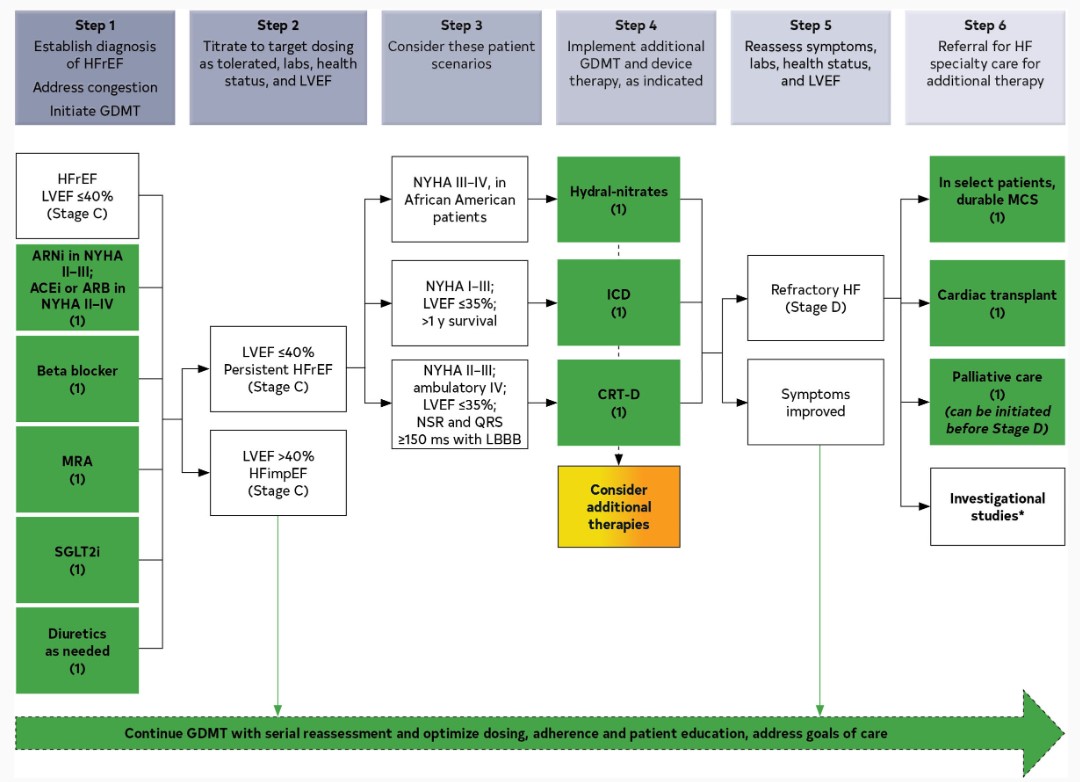
Because of the complexity of HF management and coordination of other health and social services required, HF care is ideally provided by multidisciplinary teams27–30 that include cardiologists, nurses, and pharmacists who specialize in HF as well as dieticians, mental health clinicians, social workers, primary care clinicians, and additional specialists.31–33 Self-care in HF comprises treatment adherence and health maintenance behaviors.34,35 Patients with HF should learn to take medications as prescribed, restrict sodium intake, stay physically active, and get vaccinations.36,37 They also should understand how to monitor for signs and symptoms of worsening HF, and what to do in response to symptoms when they occur.36,37 Knowledge alone is insufficient to improve self-care.38 Patients with HF need time and support to gain skills and overcome barriers to effective self-care.37 Measures listed as Class 1 recommendations for patients in stages A and B are recommended where appropriate for patients in stage C. GDMT, as depicted in Figure 6, should be the mainstay of pharmacological therapy for HFrEF.
Figure 6.Treatment of HFrEF Stages C and D. Colors correspond to COR in Table 2. Treatment recommendations for patients with HFrEF are displayed. Step 1 medications may be started simultaneously at initial (low) doses recommended for HFrEF. Alternatively, these medications may be started sequentially, with sequence guided by clinical or other factors, without need to achieve target dosing before initiating next medication. Medication doses should be increased to target as tolerated. ACEi indicates angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNi, angiotensin receptor-neprilysin inhibitor; COR, Class of Recommendation; CRT, cardiac resynchronization therapy; GDMT, guideline-directed medical therapy; ICD, implantable cardioverter-defibrillator; hydral-nitrates, hydralazine and isosorbide dinitrate; HFrEF, heart failure with reduced ejection fraction; LBBB, left bundle branch block; MCS, mechanical circulatory support; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist; NSR, normal sinus rhythm; NYHA, New York Heart Association; and SGLT2i, sodium-glucose cotransporter 2 inhibitor. *Participation in investigational studies is appropriate for stage C, NYHA class II and III HF.
Synopsis
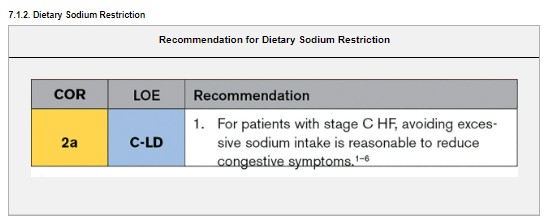
Restricting dietary sodium is a common nonpharmacological treatment for patients with HF symptomatic with congestion, but specific recommendations have been based on low-quality evidence.7 Concerns about the quality of data regarding clinical benefits or harm of sodium restriction in patients with HF include the lack of current pharmacological therapy, small samples without sufficient racial and ethnic diversity, questions about the correct threshold for clinical benefit, uncertainty about which subgroups benefit most from sodium restriction,7,8 and serious questions about the validity of several RCTs in this area.9–11 However, there are promising pilot trials of sodium restriction in patients with HF3,5,6 The AHA currently recommends a reduction of sodium intake to <2300 mg/d for general cardiovascular health promotion12; however, there are no trials to support this level of restriction in patients with HF.13 Sodium restriction can result in poor dietary quality with inadequate macronutrient and micronutrient intake.14 Nutritional inadequacies have been associated with clinical instability,15–17 but routine supplementation of oral iron,18 thiamine,19 zinc,20 vitamin D,21 or multivitamins has not proven beneficial.22 The DASH diet is rich in antioxidants and potassium, can achieve sodium restriction without compromising nutritional adequacy when accompanied by dietary counseling,5 and may be associated with reduced hospitalizations for HF.23
Synopsis
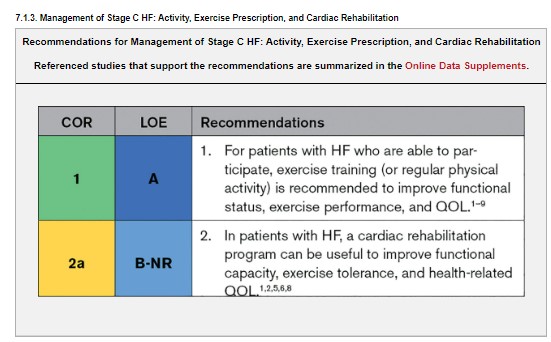
Exercise training in patients with HF is safe and has numerous benefits. In a major trial of exercise and HF, exercise training was associated with a reduction in CVD mortality or hospitalizations in the exercise training group after adjustment for risk factors.1 Meta-analyses show that cardiac rehabilitation improves functional capacity, exercise duration, and health-related QOL. A cardiac rehabilitation program for patients with HF usually includes a medical evaluation, education regarding the importance of medical adherence, dietary recommendations, psychosocial support, and an exercise training and physical activity counseling program. Patients with HF on optimal GDMT, who are in stable medical condition and are able to participate in an exercise program, are candidates for an exercise rehabilitation program.10,11
7.2. Diuretics and Decongestion Strategies in Patients With HF
Synopsis
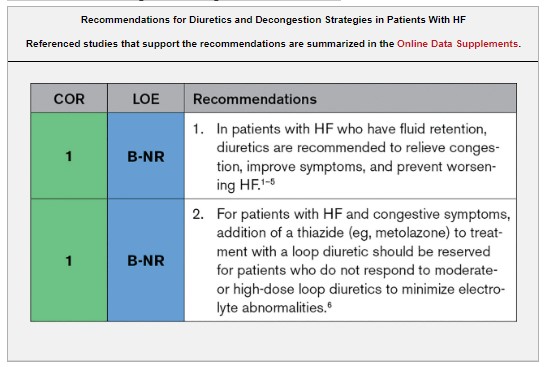
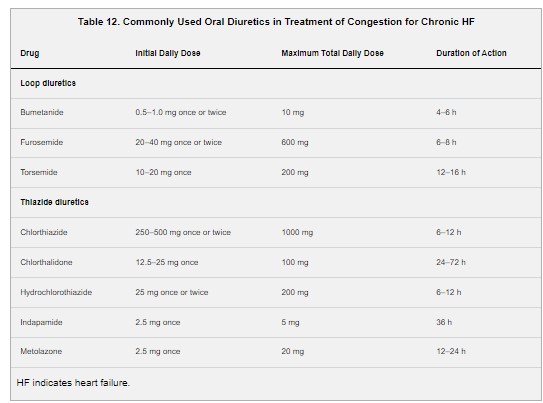
Bumetanide, furosemide, and torsemide inhibit reabsorption of sodium or chloride at the loop of Henle, whereas thiazide and thiazide-like diuretics act in the distal convoluting tubule and potassium-sparing diuretics (eg, spironolactone) in the collecting duct.7,8 Loop diuretics are the preferred diuretic agents for use in most patients with HF. Thiazide diuretics such as chlorthalidone or hydrochlorothiazide may be considered in patients with hypertension and HF and mild fluid retention. Metolazone or chlorothiazide may be added to loop diuretics in patients with refractory edema unresponsive to loop diuretics alone. Diuretics should be prescribed to patients who have evidence of congestion or fluid retention. In any patient with a history of congestion, maintenance diuretics should be considered to avoid recurrent symptoms. The treatment goal of diuretic use is to eliminate clinical evidence of fluid retention, using the lowest dose possible to maintain euvolemia. With the exception of MRAs, the effects of diuretics on morbidity and mortality are uncertain.1–5 As such, diuretics should not be used in isolation but always combined with other GDMT for HF that reduces hospitalizations and prolongs survival. Table 12 lists oral diuretics recommended for use in the treatment of chronic HF. Hyponatremia complicates HF management. If reversing potential causes and free water restriction do not improve hyponatremia, vasopressin antagonists may be helpful in the acute management of volume overload to decrease congestion while maintaining serum sodium.
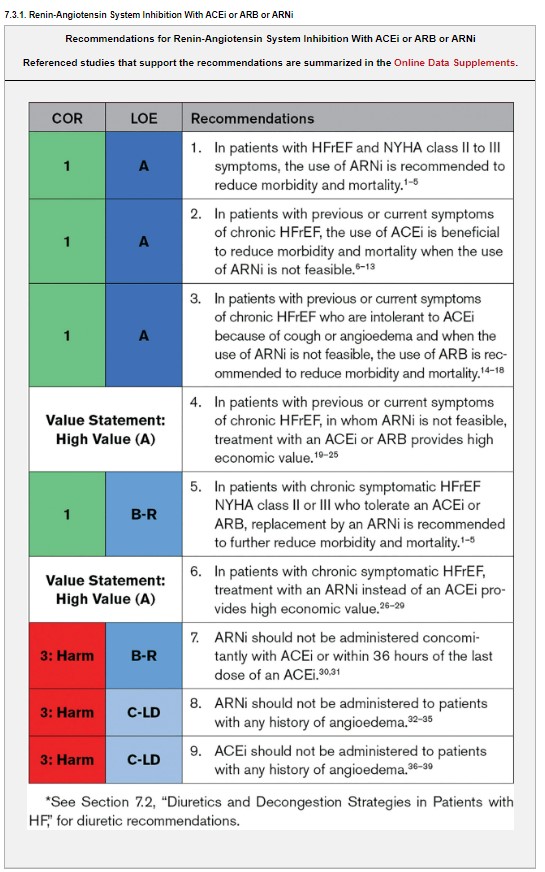
7.3. Pharmacological Treatment* for HFrEF
Synopsis
Inhibition of the renin-angiotensin system is recommended to reduce morbidity and mortality for patients with HFrEF, and ARNi, ACEi, or ARB are recommended as first-line therapy.1–18 If patients have chronic symptomatic HFrEF with NYHA class II or III symptoms and they tolerate an ACEi or ARB, they should be switched to an ARNi because of improvement in morbidity and mortality.1–5 An ARNi is recommended as de novo treatment in hospitalized patients with acute HF before discharge given improvement in health status, reduction in the prognostic biomarker NT-proBNP, and improvement of LV remodeling parameters compared with ACEi/ARB. Although data are limited, the use of an ARNi may be efficacious as de novo treatment in patients with symptomatic chronic HFrEF to simplify management. ARB may be used as an alternative to ACEi in the setting of intolerable cough, or as alternatives to ACEi and ARNi in patients with a history of angioedema. If patients are switched from an ACEi to an ARNi or vice versa, there should be at least 36 hours between ACEi and ARNi doses.
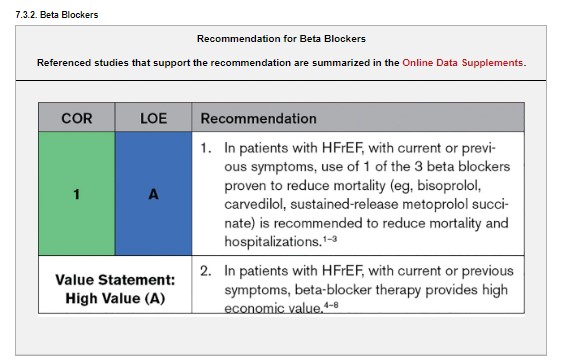
Synopsis
Treatment with beta blockers reduces the risk of death and the combined risk of death or hospitalization in patients with HFrEF.1–3 In addition, this treatment can improve LVEF, lessen the symptoms of HF, and improve clinical status.1–3,9–11 Clinical trials have shown that beta blockers should be prescribed to all patients when HFrEF is diagnosed, including in-hospital, unless contraindicated or not tolerated.1–3,9–11 These benefits of beta blockers were observed in patients with or without CAD, and in patients with or without diabetes, older patients, as well as in women and across racial and ethnic groups but not in patients with AF.1–3,10–12 Even if symptoms do not improve, long-term treatment should be maintained to reduce the risk of major cardiovascular events. Beta blockers should be initiated at low doses, and every effort should be made to achieve the target doses of the beta blockers shown to be effective in major clinical trials, as tolerated1–3,9,10 (see Section 7.3.8, “GDMT Dosing, Sequencing and Uptitration”).
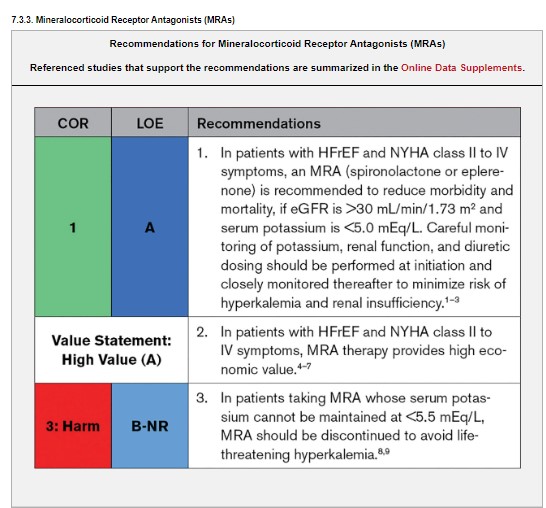
Synopsis
MRA (also known as aldosterone antagonists or anti-mineralocorticoids) show consistent improvements in all-cause mortality, HF hospitalizations, and SCD across a wide range of patients with HFrEF.1–3 Patients at risk for renal dysfunction or hyperkalemia require close monitoring, and eGFR ≤30 mL/min/1.73 m2 or serum potassium ≥5.0 mEq/L are contraindications to MRA initiation.10,11 Because of the higher selectivity of eplerenone for the aldosterone receptor, adverse effects such as gynecomastia and vaginal bleeding are observed less often in patients who take eplerenone than in those who take spironolactone.
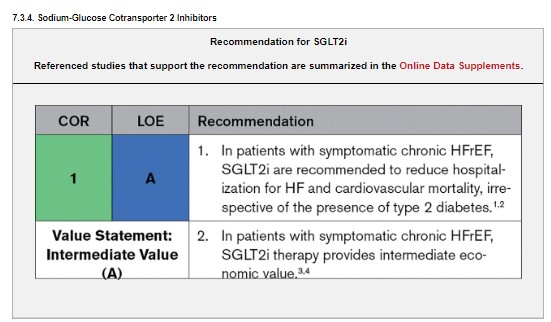
Synopsis
Several RCTs in patients with type 2 diabetes and either established CVD or high risk for CVD have shown that SGLT2i prevent HF hospitalizations compared with placebo.5–7 The overall 31% reduction in HF hospitalizations was noted irrespective of the presence or absence of preexisting HF, although only 10% to 14% of participants had HF at baseline. The benefit appears independent of the glucose-lowering effects.8 Therefore, several trials were launched to examine the efficacy of SGLT2i on outcomes in patients with HF, irrespective of the presence of type 2 diabetes. The DAPA-HF (Dapagliflozin and Prevention of Adverse Outcomes in Heart Failure) trial and EMPEROR-Reduced (EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Reduced Ejection Fraction) showed the benefit of SGLT2i (dapagliflozin and empagliflozin, respectively) versus placebo on outcomes (median follow-up, 16–18 months).1,2 Patients enrolled had symptomatic chronic HFrEF (LVEF ≤40%, NYHA class II to IV, and elevated natriuretic peptides) and were already on GDMT. Important exclusions were eGFR <20 (EMPEROR-Reduced) or <30 mL/min/1.73 m2 (DAPA-HF), type 1 diabetes, or lower SBP <95 to 100 mm Hg.
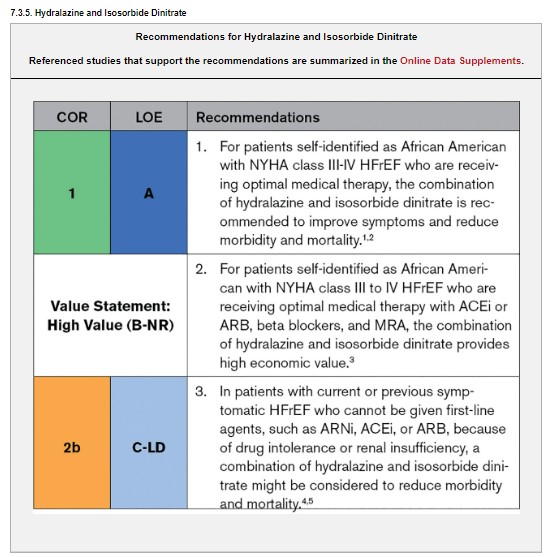
Synopsis
Two RCTs, V-HeFT I (Vasodilator Heart Failure Trial) and A-HeFT (African-American Heart Failure Trial), established benefit of the combination of hydralazine-isosorbide dinitrate in self-identified African Americans.2,4 A-HeFT was terminated early because of evidence of remarkable benefit, but the result is vulnerable to a small number of events and the exigencies of early cessation of RCTs.2 The benefit in both trials was seen only at doses achieved in those trials that are higher than doses typically used in clinical practice and with short-acting nitrate therapy.2,4 Uptake of this regimen has been modest as a result of the complexity of the medical regimen and the array of drug-related adverse effects.5 Even when prescribed, there is marked underusage based on very low prescription refill rates. Race-based medical therapy remains a challenging issue, as well, with ongoing research now focused on biological hypotheses, particularly absence of European ancestry, which may be associated with responsiveness to this combination. There are insufficient data to guide the use of hydralazine-isosorbide dinitrate with ARNi. In patients with HFrEF who cannot receive first-line agents such as ARNi, ACEi, or ARB, referral to a HF specialist can provide guidance for further management because the use of hydralazine and isosorbide dinitrate in these patients is uncertain.
Synopsis
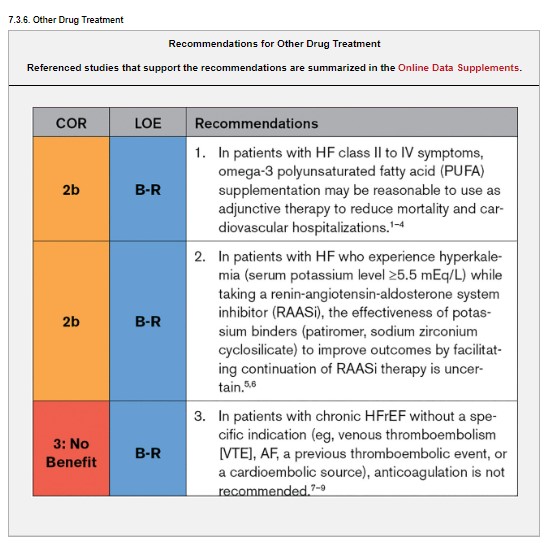
Trials in prevention of CVD, including HF, showed that omega-3 PUFA supplementation results in a 10% to 20% risk reduction in fatal and nonfatal cardiovascular events when used with other evidence-based therapies.2,3,10 Hyperkalemia is common in HF and can lead to arrhythmias and underuse of GDMT.11,12 Two newer gastrointestinal potassium-binding agents—patiromer and sodium zirconium cyclosilicate—have been shown to lower potassium levels and enable treatment with a RAASi in patients with HF.5,6,13
Synopsis
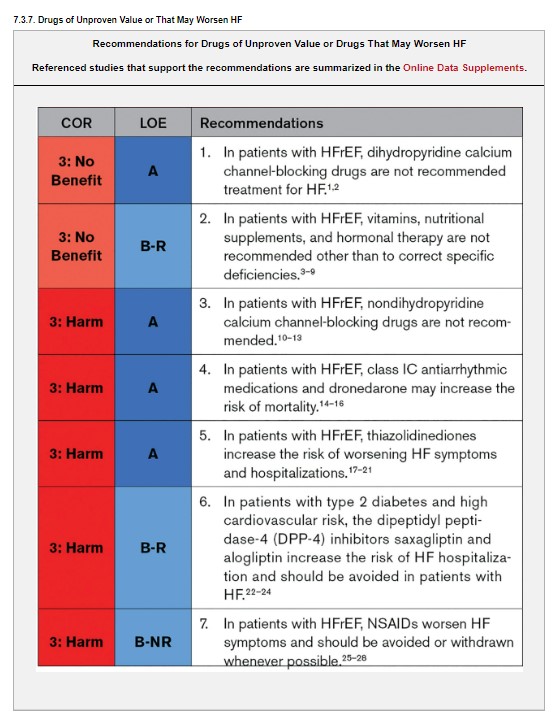
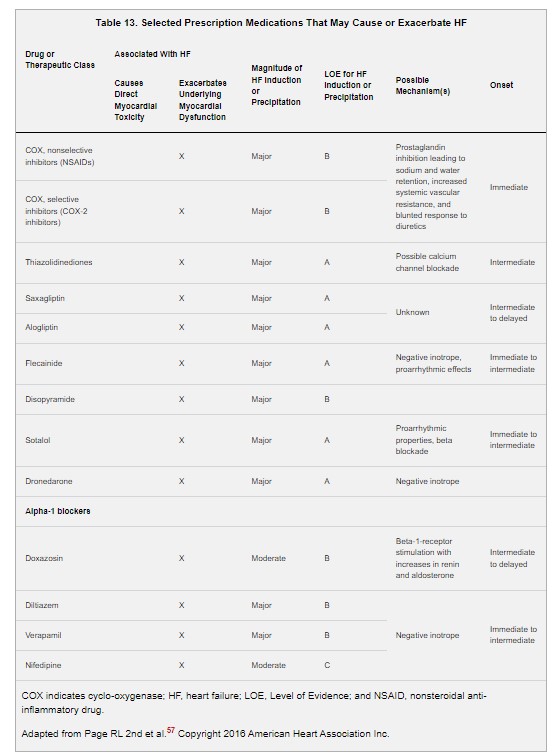
Although there is strong evidence for benefit with selected medications for HFrEF as outlined in Section 7.3, “Pharmacological Treatment for HF With Reduced Ejection Fraction (HFrEF),” there remain several classes of medications that have either unproven value or potential for harm (Table 13). These recommendations are not exhaustive but focus on the most relevant and commonly encountered medications in the management of patients with HFrEF: calcium channel blockers; antiarrhythmic agents; NSAIDs; medications for treatment of type 2 diabetes including thiazolidinediones and DPP-4 inhibitors; and vitamins, hormones, and nutritional supplements.
Synopsis
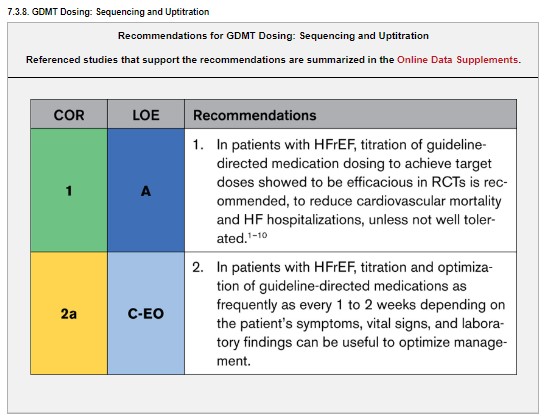
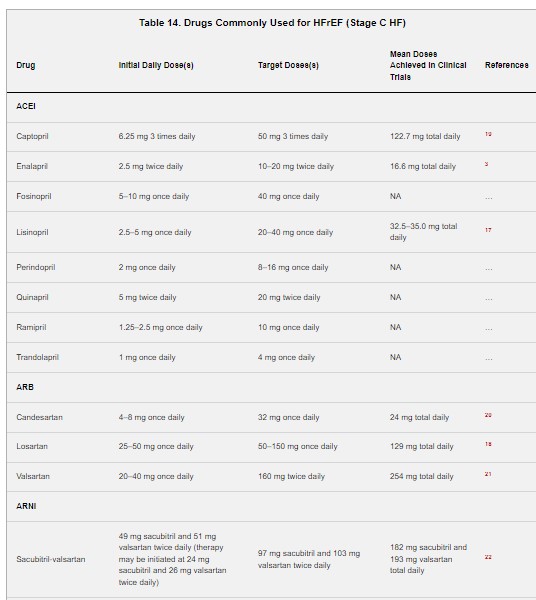
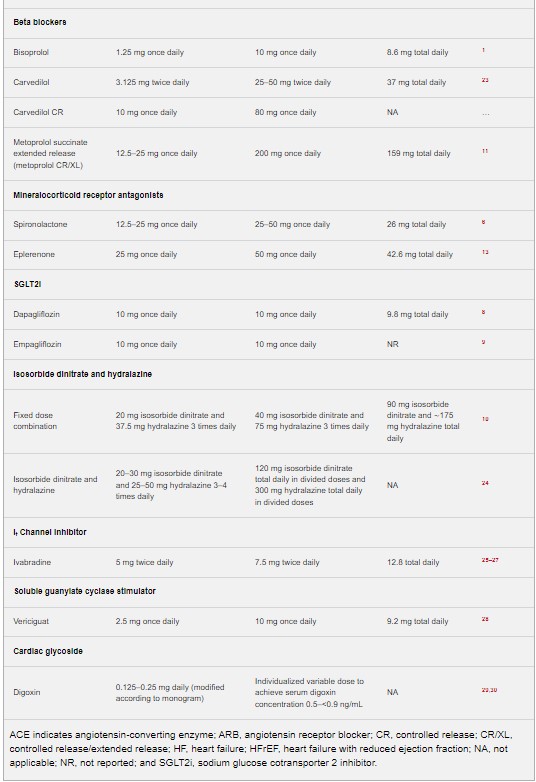
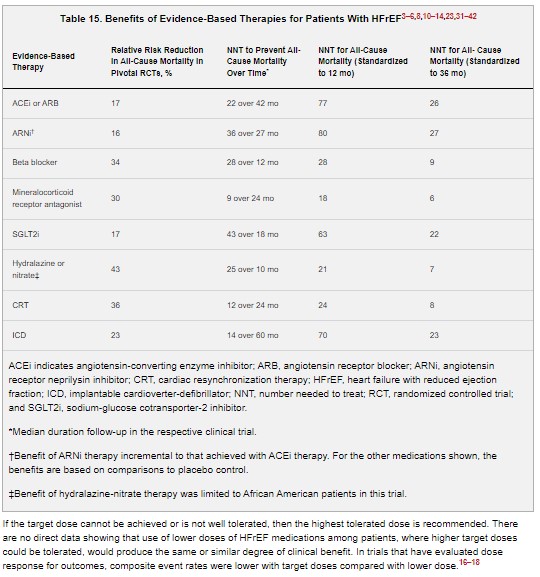
Clinical trials of ACEi, ARB, ARNi, beta blockers, and most other HFrEF medications had therapy initiated at low dose by trial protocol.1–9,11–14 If the initial dose was tolerated, the protocol would then direct the uptitration of medication dose over time to a specified target dose (Table 14), unless not well tolerated. Even if symptoms improved or other indicators of response were shown at lower doses, the medication dose would still be increased to the trial-defined target doses. Because these target doses were the ones that established the efficacy and safety of these medications in HFrEF and serve as the basis of the guideline recommendations (Table 15), use of these target doses is recommended, if tolerated.1–9,11–14 Use of all 4 drug classes has been estimated to reduce all-cause mortality by 73% compared with no treatment.15
7.3.9. Additional Medical Therapies
Synopsis
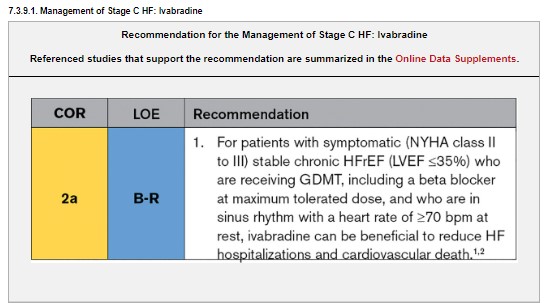
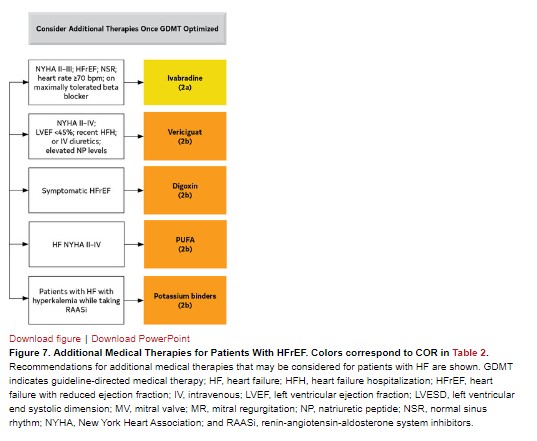
Heart rate is a strong predictor of cardiovascular outcomes in the general population and in patients with CVD, including HF. The SHIFT (Ivabradine and Outcomes in Chronic Heart Failure) trial tested the hypothesis that reducing heart rate in patients with HF improves cardiovascular outcomes.1 SHIFT demonstrated the efficacy of ivabradine, a sinoatrial node modulator that selectively inhibits the If current, in reducing the composite endpoint of cardiovascular death or HF hospitalization in patients with HF. See Figure 7 for a summary of additional medical therapy recommendations.
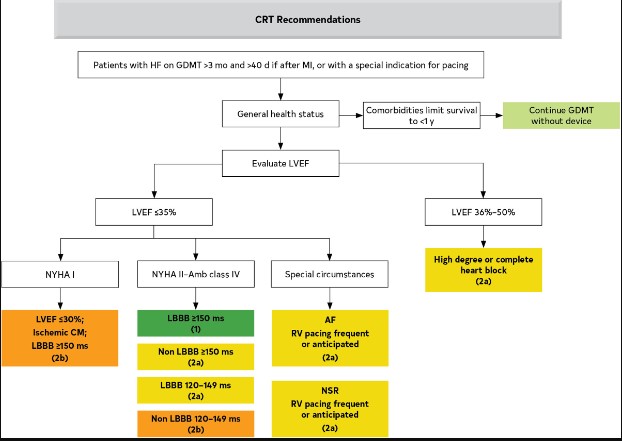
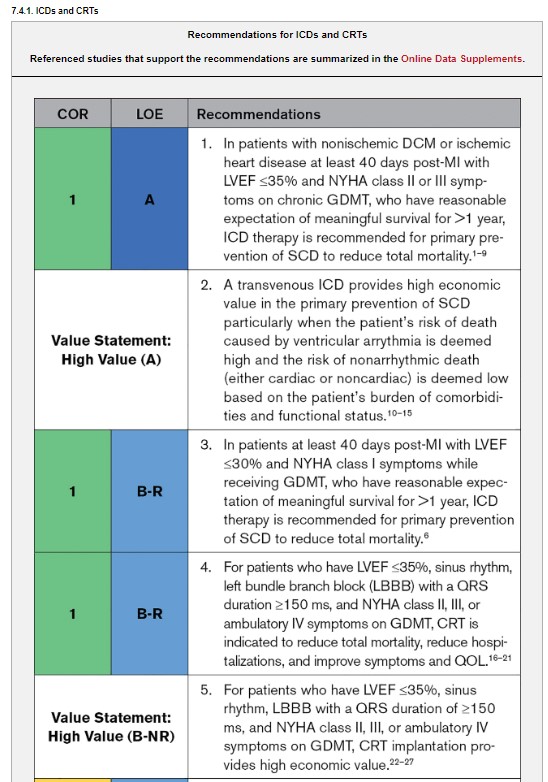
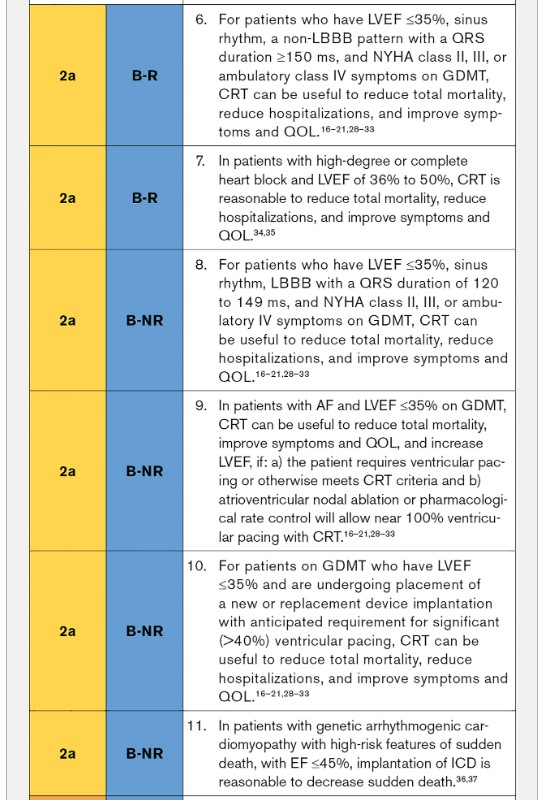
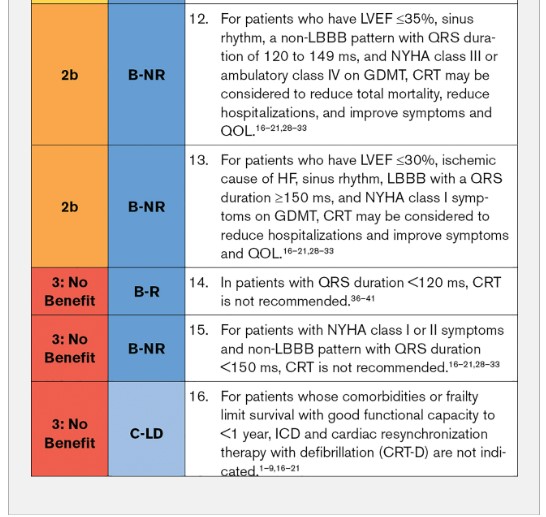
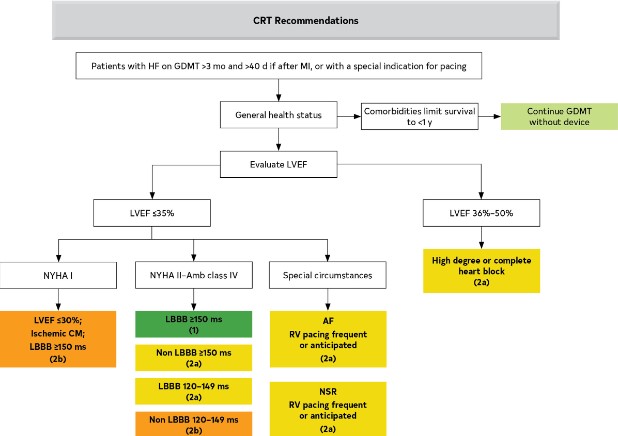
Figure 8.Algorithm for CRT Indications in Patients With Cardiomyopathy or HFrEF. Colors correspond to COR in Table 2. Recommendations for cardiac resynchronization therapy (CRT) are displayed. AF indicates atrial fibrillation; Amb, ambulatory; CM, cardiomyopathy; GDMT, guideline-directed medical therapy; HB, heart block; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; LBBB, left bundle branch block; LV, left ventricular; LVEF, left ventricular ejection fraction; NSR, normal sinus rhythm; NYHA, New York Heart Association; and RV, right ventricular.
7.3.9.2. Pharmacological Treatment for Stage C HFrEF: Digoxin
Synopsis
To date, there has been only 1 large-scale, RCT of digoxin in patients with HF.1 This trial, which predated current GDMT, primarily enrolled patients with NYHA class II to III HF and showed that treatment with digoxin for 2 to 5 years had no effect on mortality but modestly reduced the combined risk of death and hospitalization. The trial also found no significant effect on health-related QOL in a subset of the trial patients.3 The effect of digoxin on hospitalizations has been supported by retrospective analyses and meta-analyses.2,4–6 Additionally, observational studies and retrospective analyses have shown improvement in symptoms and exercise tolerance in mild to moderate HF; however, they have mostly shown either lack of mortality benefit or increased mortality associated with digoxin.7 The benefit in patients on current GDMT is unclear because most trials preceded current GDMT. Thus, use of digoxin requires caution in patients with HF and is reserved for those who remain symptomatic despite optimization of GDMT.
Synopsis
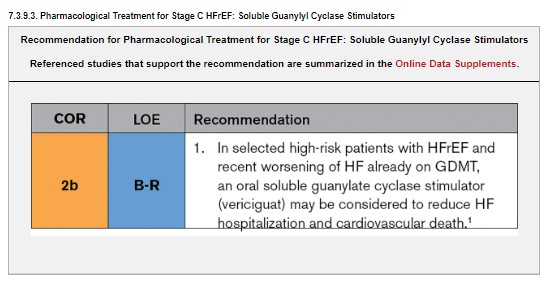
In patients with progression of HFrEF despite GDMT, there may be a role for novel therapeutic agents. Oral soluble guanylyl cyclase stimulator (eg, vericiguat) directly binds and stimulates sGC and increases cGMP production. cGMP has several potentially beneficial effects in patients with HF, including vasodilation, improvement in endothelial function, as well as decrease in fibrosis and remodeling of the heart.2–7 The VICTORIA (Vericiguat Global Study in Subjects with Heart Failure with Reduced Ejection Fraction) trial randomized 5050 higher-risk patients with worsening HFrEF to vericiguat versus placebo.1
7.4. Device and Interventional Therapies for HFrEF
Synopsis
RCTs have informed the decisions regarding cardiac implantable devices (ICDs and CRTs) over the past 20 years. In fact, the seminal RCTs for ICDs and CRTs are unlikely to be repeated. Subgroup analyses of these trials have also informed decisions, but these were not the primary endpoints of these studies and thus should be interpreted with caution. GDMT is optimized before ICD and CRT implantation to assess whether the LVEF improves. Figures 8 and 9 summarize device and interventional therapy recommendations.
Figure 8.Algorithm for CRT Indications in Patients With Cardiomyopathy or HFrEF. Colors correspond to COR in Table 2. Recommendations for cardiac resynchronization therapy (CRT) are displayed. AF indicates atrial fibrillation; Amb, ambulatory; CM, cardiomyopathy; GDMT, guideline-directed medical therapy; HB, heart block; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; LBBB, left bundle branch block; LV, left ventricular; LVEF, left ventricular ejection fraction; NSR, normal sinus rhythm; NYHA, New York Heart Association; and RV, right ventricular.
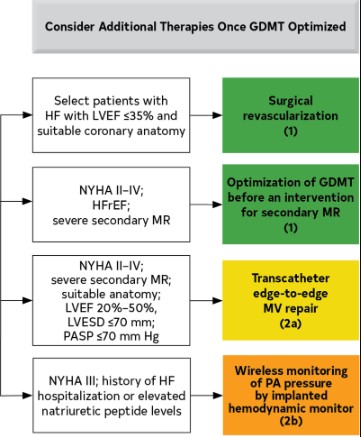
Figure 9.Additional Device Therapies. Colors correspond to COR in Table 2. Recommendations for additional nonpharmaceutical interventions that may be considered for patients with HF are shown. GDMT indicates guideline-directed medical therapy; HF, heart failure; HFH, heart failure hospitalization; HFrEF, heart failure with reduced ejection fraction; IV, intravenous; LVEF, left ventricular ejection fraction; LVESD, left ventricular end systolic dimension; MV, mitral valve; MR, mitral regurgitation; NP, natriuretic peptide; NSR, normal sinus rhythm; NYHA, New York Heart Association; and PASP, pulmonary artery systolic pressure.
Recommendation-Specific Supportive Text
1.
CABG has been shown to improve outcomes in patients with left main or left main equivalent disease and HF.1,4,10–14 Long-term follow-up shows a reduction in all-cause, cardiovascular, and HF hospitalizations and in all-cause and cardiovascular mortality in patients with LV dysfunction who receive CABG and GDMT compared with GDMT alone.2,7 The long-term survival benefit is greater in those with more advanced ischemic cardiomyopathy (lower EF or 3-vessel disease) and diminishes with increasing age.5,7 CABG also improves QOL compared with GDMT alone.3 An RCT of CABG combined with surgical ventricular remodeling compared with CABG alone did not show a reduction in death or hospitalization, or improvement in symptoms with surgical ventricular remodeling.15 Surgical ventricular remodeling performed at the time of CABG may be useful in patients with intractable HF, large thrombus, or persistent arrhythmias resulting from well-defined aneurysm or scar, if other therapies are ineffective or contraindicated.15,16
7.5. Valvular Heart Disease
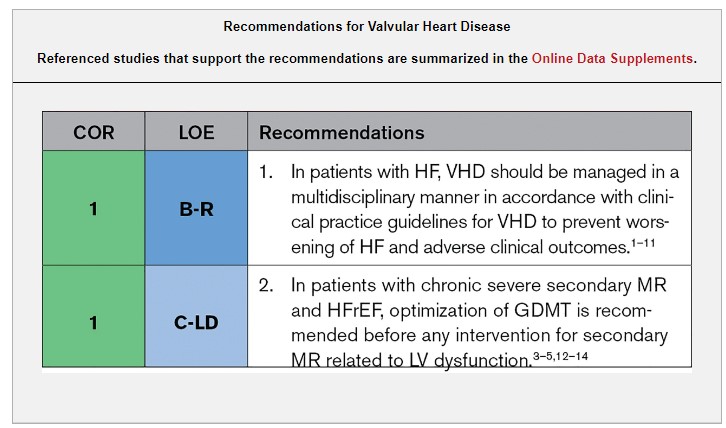
Synopsis
GDMT applies to all patients with HFrEF, irrespective of the presence of VHD. Significant valve disease warrants evaluation by a multidisciplinary team with expertise in VHD, and management should proceed in accordance with the VHD guidelines.15
7.6. Heart Failure With Mildly Reduced EF (HFmrEF) and Improved EF (HFimpHF)
Synopsis
There are no prospective RCTs for patients specifically with HFmrEF (LVEF, 41%–49%). All data for HFmrEF are from post hoc or subsets of analyses from previous HF trials with patients now classified as HFmrEF. LVEF is a spectrum, and among patients with LVEF 41% to 49%, patients with LVEF on the lower end of this spectrum appear to respond to medical therapies similarly to patients with HFrEF. Thus, it may be reasonable to treat these patients with GDMT used for treatment of HFrEF. Patients with HFmrEF should have repeat evaluation of LVEF to determine the trajectory of their disease process. Future prospective studies are needed to further clarify treatment recommendations for patients with HFmrEF. Figure 11 summarizes COR 1, 2a, and 2b for HFmrEF.