Today, I review and excerpt from the Effusion Section of
The “5Es” of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Acad Emerg Med. 2015 May;22(5):583-93. doi: 10.1111/acem.12652. Epub 2015 Apr 22.
All that follows is from the above resource.
Abstract
Emergency physician (EP)-performed focused cardiac ultrasound (EP FOCUS) has been increasingly recognized as a crucial tool to help clinicians diagnose and treat potentially life-threatening conditions. The existing literature demonstrates a variety of EP FOCUS applications and protocols; however, EP FOCUS is not taught, practiced, or interpreted consistently between institutions. Drawing on over 12 years of experience in a large-volume, high-acuity academic emergency department, we have developed a protocol for teaching and performing EP FOCUS known as “The 5Es,” where each E represents a specific assessment for immediately relevant clinical information. These include pericardial effusion, qualitative left ventricular ejection, ventricular equality, exit (aortic root diameter), and entrance (inferior vena cava diameter and respirophasic variation). Each of these assessments has been well described in the emergency medicine literature and is within the scope of EP-performed echocardiography. This approach provides a reliable and easily recalled framework for assessing, teaching, and communicating EP FOCUS findings that are essential in caring for the patient in the emergency setting.
Effusion
The first “E” in our protocol is an assessment for pericardial effusion. Of the echo components in our protocol, detection of pericardial effusion was the first to be clearly investigated and delineated in the literature and has been incorporated as part of the FAST for more than 20 years.1, 2, 10, 11 Given the wide range of symptoms and the potential for hemodynamic collapse, timely and accurate detection of a pericardial effusion is essential for expediting diagnosis and management.12 EP FOCUS can identify pericardial effusions at the bedside with a high degree of diagnostic accuracy.13 EP FOCUS has been shown to improve mortality in penetrating cardiac trauma.14 In a study of emergency department (ED) patients with unexplained dyspnea, more than 10% were found to harbor pericardial effusions.15 Tamponade physiology is detectable earlier with US than with traditional exam findings, such as Beck’s triad.13, 16
Pericardial effusions may be characterized as focal, circumferential, simple, or complex. While circumferential effusions are most common, it is important to obtain as many views as possible so as not to miss a focal effusion. This is of particular importance following any invasive cardiac procedure. Complex effusions (with internal echoes) may occur in the presence of pericardial hemorrhage or infectious effusions or in long-standing effusions with fibrous stranding. Of note, while uncommon in the developed world, tuberculosis is the most common cause of pericardial effusion in the developing world and often presents with complex effusions.17
Techniques for Assessing Effusion
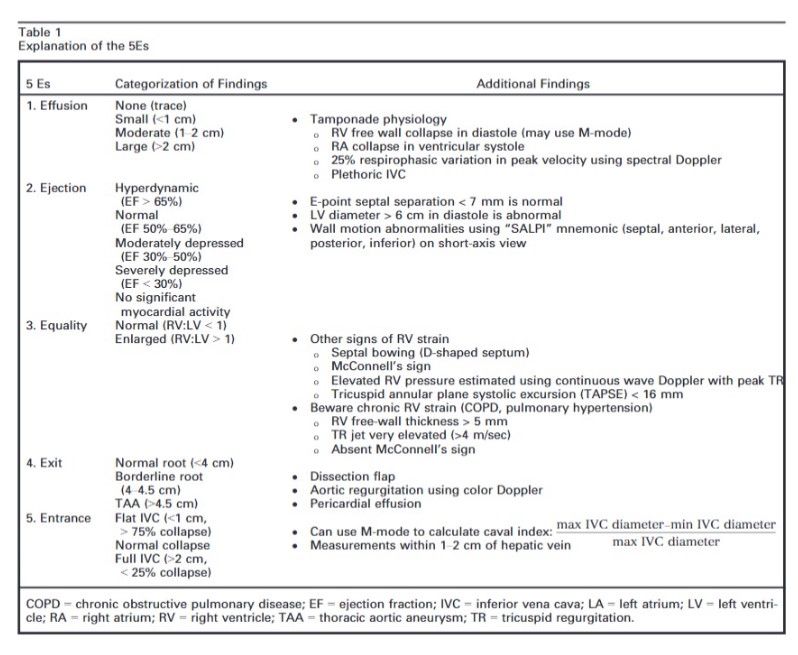
The subcostal window (either SC4C or SCLA) is the most reliable view for detecting pericardial effusions because the most dependent portion of the pericardium is closest to the face of the probe. In this window, the liver can also help provide an acoustic window to the inferior pericardium. In the parasternal views (PSLA and PSSA), significant effusions should be visualized posterior to the left ventricle (LV) and not just anteriorly, as this will often be a fat pad and not an effusion (Figure 1). In the A4C view, small effusions may be visible lateral to the LV free wall, and moderate to large effusions may be seen tracking completely around the apex of the heart.
Normal patients have a trace amount physiologic pericardial fluid that may be seen with modern equipment and described as trivial or “not clinically significant.” True effusions can be categorized as “small,” “moderate,” or “large.” This categorization is often qualitative, although an effusion can be measured by assessing the largest pocket of fluid at end-diastole and measured orthogonally to the surface of the heart. By convention, small effusions are smaller than 1 cm, moderate effusions are 1 to 2 cm, and large effusions are >2 cm.18 Moderate to large effusions are more likely to have an effect on hemodynamics; however, even small effusions can also result in tamponade physiology.19, 20 Prognosis in the setting of pericardial effusion is largely related to time course and etiology, and it is important to recognize that the hemodynamic sequelae of an effusion is much more important than its actual size.18, 21
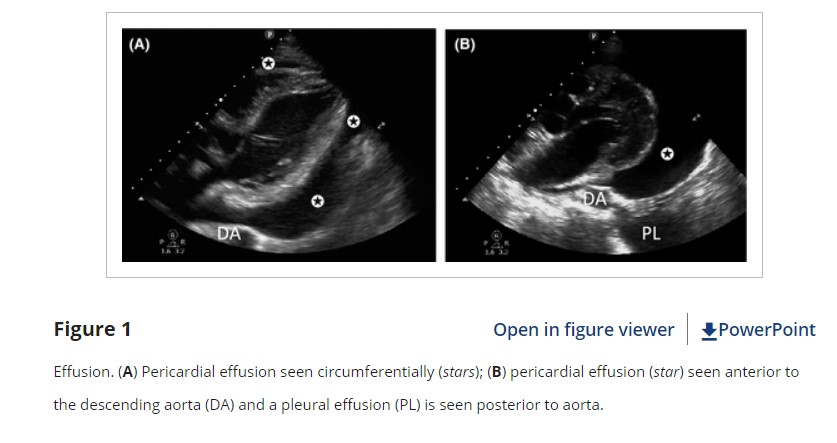
Identification of an effusion should prompt the practitioner to look for signs of tamponade physiology. As pressures inside the pericardium elevate, US will show a progression of findings beginning with collapse of the right atrium (RA), collapse of the right ventricle (RV), and finally LV collapse.20 One of the most easily obtained and sensitive signs of tamponade is the presence of a noncollapsible, plethoric IVC (the fifth “E”), indicating impaired filling from extrinsic compression of the heart.22 Collapse of the RA in ventricular systole or the RV in diastole indicates tamponade physiology, but tachycardia may make it difficult to differentiate normal systolic ventricular collapse from pathologic diastolic ventricular collapse. To confirm RV diastolic collapse, M-mode can be used in either the PSLA or SX4C views to demonstrate RV free wall motion as it relates to the anterior leaflet of the mitral valve (Figure 2). If the RV free wall is collapsed when the mitral (anterior) valve is open, it indicates diastolic collapse of the RV.
Tamponade physiology can also be demonstrated on echo by exaggerated respiratory variation of ventricular in-flow velocities (the echo equivalent of pulsus paradoxus).23 In an A4C view, a pulsed wave spectral Doppler gate is placed at the tips of the mitral valve during diastole. A change of more than 25% in the early filling signal (“E wave”) indicates impaired filling (Figure 2). While these techniques can help determine the presence of tamponade physiology, they are not completely sensitive or specific and should be used in conjunction with clinical judgment.
Pearls and Pitfalls for Effusion
A common pitfall, particularly among novice practitioners of EP FOCUS, is confusing epicardial or pericardial fatty tissue for an effusion.24 Fatty tissue can be characterized by its heterogeneous echo-texture, its coordinated movement in conjunction with the myocardium, and its failure to track around the heart, especially at the apex and posteriorly. A false-positive diagnosis may occur when a hypoechoic space is seen only anterior to the heart on the PSLA view. In the parasternal views, pathologic effusions are typically visible posteriorly, in the most dependent portion of the pericardium (Figure 1). Most clinically significant effusions will not obliterate during diastole and can be traced with US around the apex of the heart and/or posteriorly. Exceptions are loculated or focal effusions and therefore multiple views are recommended.
It should be noted that there are other causes of RA and RV diastolic collapse, including severe hypovolemia and large pleural effusions. Pleural effusions may be misinterpreted as pericardial effusions, particularly in the PSLA window where left-sided pleural fluid lies adjacent to the LV. They can be differentiated by their relationship to the descending aorta. Pericardial effusions will track between the descending aorta and the LV free wall, while pleural effusions will track posterior and lateral to the descending aorta (Figure 1).
Due to the nonspecific clinical presentations of pericardial effusion and tamponade, we recommend having a low threshold for employing US, particularly when a patient presents with unexplained dyspnea, tachycardia, hypotension, near-syncope, or cardiomegaly on chest radiograph. While visualization of the pericardium is essential in the initial evaluation of penetrating thoracoabdominal trauma, pericardial effusion as a result of blunt trauma is rare, and such patients are unlikely to survive to ED presentation.23 The identification of a pericardial effusion in blunt trauma should raise the suspicion of either a false-positive or an incidental pericardial effusion and should not necessarily indicate the need for acute intervention unless there is severe hemodynamic compromise without another source.
Conclusions
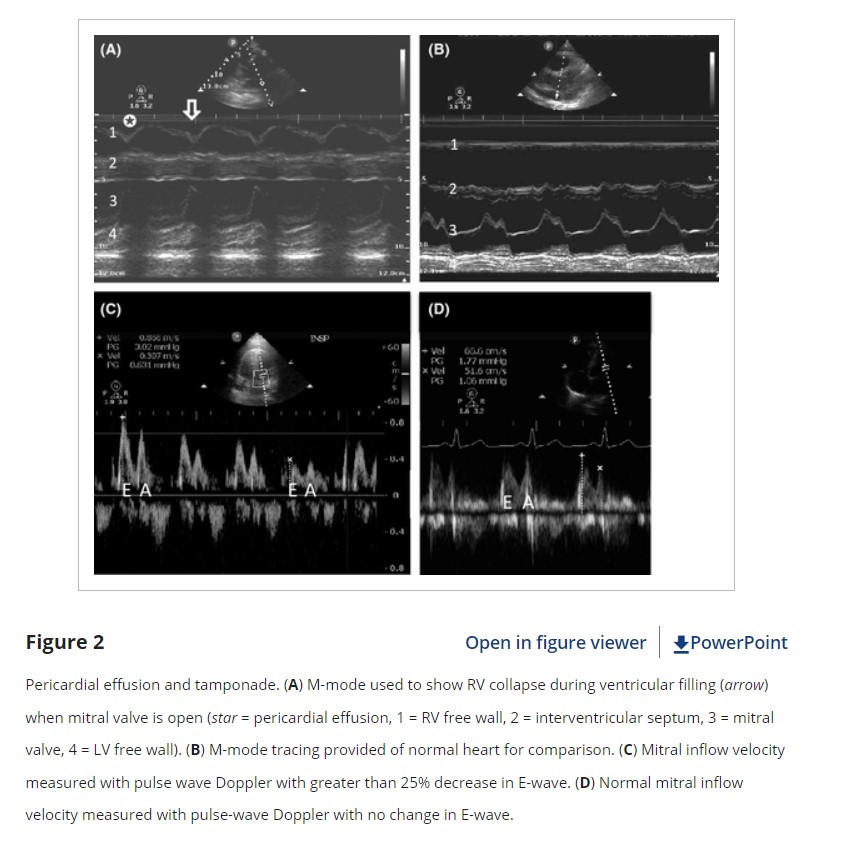
The intent of this article is to codify elements of the cardiac US exam that we have found to be most relevant to patients presenting with acute or emergent complaints (Table 1). A recent international consensus statement defined FOCUS as being goal-directed, problem-oriented, limited in scope, simplified, time-sensitive and repeatable, qualitative and semiquantitative, performed at the point of care, and usually performed by clinicians.6 The 5Es described in this article meet all of these criteria. However, the international statement addressed the use of FOCUS in “all clinical settings” and included the assessment of chronic cardiac disease, as well as gross valvular abnormalities and large intracardiac masses, without assessment of the thoracic aorta.
In our experience the 5Es encompass the cardiac US findings most applicable in patients who present emergently with hypotension, dyspnea, syncope, penetrating thoracic trauma, chest pain, or other acute complaints where diagnosis may be aided by visualization of the heart. While gross valvular abnormalities and intracardiac masses are important if they are seen, they are less common and less acute and tend to be less immediately deadly than acute thoracic aortic disease, which accounts for more than twice as many deaths as abdominal aortic aneurysm rupture.51The 5Es are not meant to provide an absolute boundary for EP FOCUS, which will likely continue to evolve, but are intended to provide a framework for the acquisition and interpretation of the most relevant and applicable components of echocardiography in the emergent setting. We hope that adoption and subsequent application of the 5Es in EDs will help to standardize and effectively teach the echo findings that may allow EPs to save lives and expedite the care of patients with potentially life-threatening illness.We thank Jane Hall, PhD, for preparing Figures 4, 6, and 8. We also thank Daniel Wadsworth Groves, MD, for manuscript review.