
The podcast, Ep 106 Toxic Alcohols – Minding the Gaps [Link is to the show notes and podcast], from Emergency Medicine Cases is outstanding [I know I always say that – but it is always true]
For much more on anion gap metabolic acidosis, please see my post,The new GOLDMARK Mnemonic For Anion Gap Metabolic Acidosis From Emergency Medicine Cases posted on July 13, 2017 .
And here is the Introduction from the HTML shownotes of Episode 106 [but again don’t be fooled, you MUST listen to the complete podcast and review the complete shownotes to get the maximum benefit for your patients]:
Dr. Helman’s Introduction:
We see patients with toxic alcohol poisoning most commonly in three clinical scenarios. One, which is usually relatively straightforward, after an intentional suicide attempt where they tell you exactly what they took; the next scenario is a bit more challenging – when they come in agitated and won’t give you a history and the third – also very challenging – the inebriated patient found down. Alcohol is everywhere, and inevitably inebriated people show up at your ED with a myriad of medical and psychiatric problems – we’re all familiar with these patients. Or they are simply very drunk. And most of them just need to sober up and can be sent home. But, it’s our job as ED professionals, not only to identify traumatic, medical and psychiatric catastrophes in these patients but also to identify and manage the relatively rare but potentially life and sight threatening toxicologic diagnoses in the inebriated or agitated patient. And that isn’t so easy – especially when it comes to toxic alcohols.
So, in this Episode #106 Toxic Alcohols – Minding the Gaps – Recognition and Emergency Management, we’ve got the mighty return of two of my favorite brilliant Toronto based toxicologists –Margaret Thompson, the medical director of the Ontario Poison Control Centre, and the blossoming toxicology educator extraordinaire Emily Austin to help give you the knowledge of toxic alcohol poisoning recognition, clinical and lab clues, limitations of the osmolar gap, goals of management, time sensitive treatments and more…
What follows are some excerpts from the PDF show notes of this episode [sometimes the HTML show notes and the PDF show notes differ]:
Episode 106 Toxic Alcohols – Minding the
Gaps
With Margaret Thompson & Emily Austin
Prepared by Anton Helman, January 2018
And here is Dr. Helman’s outstanding summary the take home points of the podcast from the PDF show notes:
Take home points for toxic alcohol poisoning
Recognition: Clinical clues
1. Tachypnea in absence of respiratory illness caused by
patient’s effort to blow off CO2 with metabolic acidosis
2. Visual changes
3. Not sobering up as expected
4. SeizureRecognition: Lab clues
1. AG metabolic acidosis (caused by toxic alcohol +/- elevated
lactate and renal failure)
2. High osmolality +/- osmolar gap (note that osmolality
decreases with time)
3. Low ethanol level in intoxicated patient
4. Hypocalcemia with prolonged QT
5. Bilateral basal ganglia hemorrhages on CT (late finding)Goals of Management
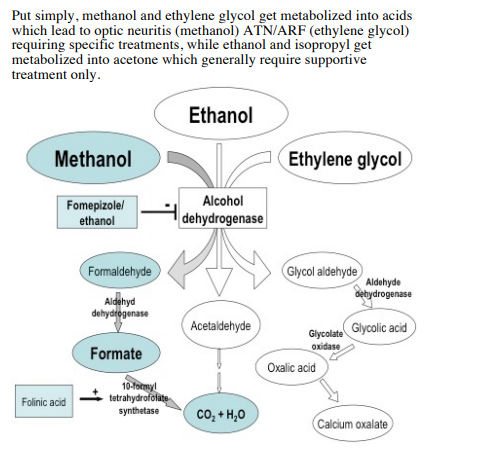
1. Block the toxic metabolites with fomepizole or ethanol
2. Correct pH to 7.2 with bicarb
3. Eliminate toxic metabolites with dialysis (esp methanol)Time sensitive management actions
1. Airway – consider DSI with ketamine, match pre-intubation
respiratory rate with post intubation respiratory rate and
consider bicarbonate boluses to avoid worsening acidosis
and cardiovascular collapse
2. Call poison control center +/- nephrology early 3. Consider fomepizole or ethanol to block toxic metabolites
4. Bicarbonate infusion to correct acidosis to pH = 7.2
5. Replenish cofactors
6. Consider dialysis in almost all methanol and some ethylene
glycol poisoning



