
This post is just my study notes (my peripheral brain) on the evaluation of syncope. I find that creating these posts really helps me fix the subject in my mind and helps me when I want to do a rapid review.
Primary care physicians in many practice settings (office, urgent care, and emergency department) may all be called upon to evaluate syncope. Just as TIA can be a warning of an increased risk of stroke, so can syncope be a warning sign of an increased risk of sudden death.
Thus, careful evaluation of syncope is critical to prevention of the tragedy of sudden death no matter what your practice setting is.
Resources (1) through (4) provide the best framework for the evaluation of syncope that I have seen.
The following are some excerpts from Resource (1):
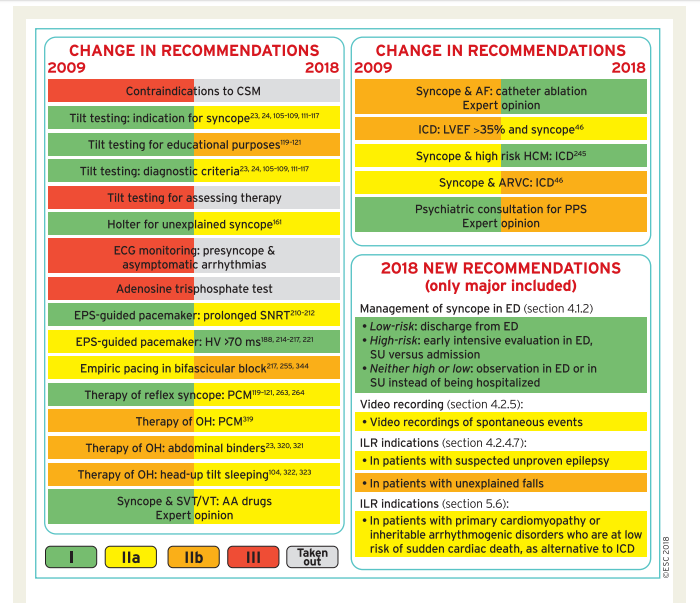
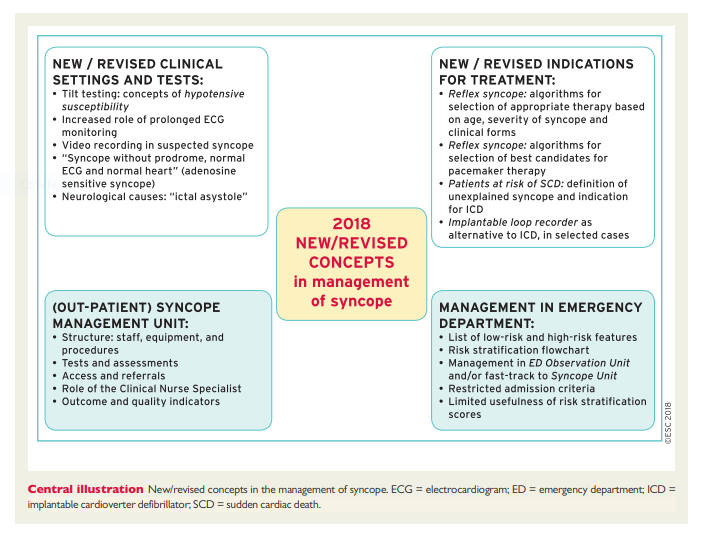
Compared with the previous versions of these Guidelines, the 2018 document contains Supplementary Data as an integral part. While the print text mainly aims to give formal evidence-based recommendations according to the standardized rules of the ESC, this new web-only feature allows expansion of the content to practical issues, and aims to fill the gap between the best available scientific evidence and the need for dissemination of these concepts into clinical practice (‘We have the knowledge, we need to teach it’). Thanks to the Supplementary Data further explanation on specific points is given, and thanks to the Web Practical Instructions advice is given on how to evaluate patients with loss of consciousness (LOC), and how to perform and interpret tests properly; whenever possible, we provide tracings, videos, flow charts, and checklists.
The document aims to be patient-orientated and focused on therapy, and to reduce the risk of recurrence and the life-threatening consequences of syncope recurrence. For this purpose, even in the absence of strong evidence from trials, we give as much advice as possible on the most appropriate therapy based on the practical expertise of the members of the Task Force (‘Our patients seek solutions, not only explanations’). When possible, we provide therapeutic and decision-making algorithms.
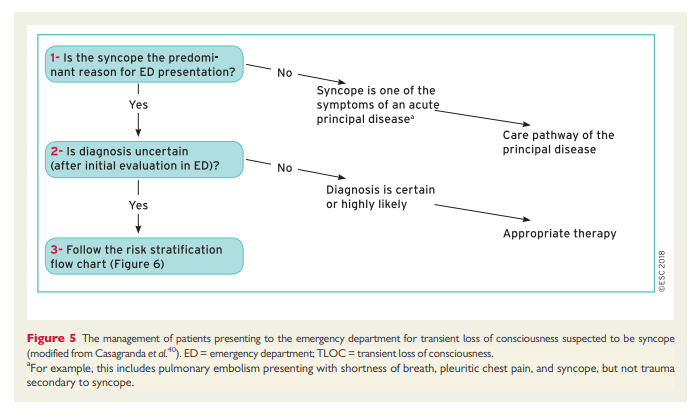
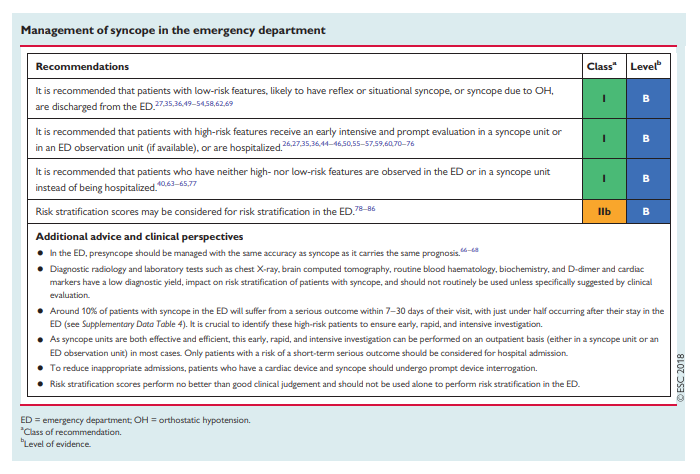
Finally, we recognize that one major challenge in syncope management is the reduction of inappropriate admissions and inappropriate use of tests while maintaining the safety of the patient. We give strong focus to pathways and organizational issues (‘We have the knowledge; we need to apply it’). In particular, we propose a care pathway for the management of patients with TLOC from their arrival in the emergency department (ED), and give practical instructions on how to set up outpatient syncope clinics (syncope units) aimed at reducing hospitalization, under- and misdiagnoses, and costs.
4.2.1 Carotid sinus massage
A ventricular pause lasting >3 s and/or a fall in systolic BP of >50 mmHg is known as carotid sinus hypersensitivity. Carotid sinus hypersensitivity is a common finding in older men without syncope; abnormal responses are frequently observed (≤40%) in patients without syncope, especially if they are older and affected by cardiovascular disease.89 Carotid sinus hypersensitivity is exceptional in patients <40 years of age.90 The specificity of the test increases if spontaneous syncope is reproduced during CSM. Syncope was induced in only 5% of asymptomatic persons aged >65 years.89 For the above reasons, the diagnosis of carotid sinus syndrome (CSS) requires the reproduction of spontaneous symptoms and, in addition, that patients have syncope of unknown origin compatible with a reflex mechanism. In such circumstances, CSM usually shows a period of asystole >6 s.91 The prevalence of CSS, as defined here, was 8.8% when CSM was performed after the initial evaluation in 1855 consecutive patients >40 years of age with syncope compatible with a reflex mechanism.92,93 In a multicentre study94 aimed at validation of the 2009 ESC Guidelines, CSM was indicated after initial evaluation in 73% of 700 patients and was diagnostic in 12%. The precise methodology and results of CSM are shown in section 5 of the Web Practical Instructions.
The main complications of CSM are neurological. When pooling the data from four studies90,95–97 in which 8720 patients were analysed, TIAs or strokes were observed in 21 (0.24%).
The relationship between abnormal response to CSM and spontaneous syncope is a crucial point that has been studied using two methods. The first was a pre−post comparison of the recurrence rate of syncope after pacing. Non-randomized studies demonstrated fewer recurrences at follow-up in paced patients than in those without pacing. These results were confirmed in two randomized trials.98,99 The second method was to analyse the occurrence of asystolic episodes registered in patients with a cardioinhibitory response to CSM using an implanted device. Recordings of long pauses were very common in the two trials that employed this method.100,101 These results suggest that a positive response to CSM, reproducing symptoms, in patients with syncope is highly predictive of the occurrence of spontaneous asystolic episodes.
There is strong consensus that the diagnosis of CSS requires both the reproduction of spontaneous symptoms during CSM and clinical features of spontaneous syncope compatible with a reflex mechanism. The quality of evidence is moderate and is given by studies of ECG correlation between CSM and spontaneous events, and indirectly by studies of efficacy of cardiac pacing. Further research is likely to have an important impact on our confidence in the estimation of effect and may change the estimate.
4.2.2 Orthostatic challenge
Changing from the supine to the upright position produces a displacement of blood from the thorax to the lower limbs and abdominal cavity that leads to a decrease in venous return and cardiac output. In the absence of compensatory mechanisms, a fall in BP may lead to syncope.20,103,104 The diagnostic criteria for OH have been defined by consensus.6
Currently, there are three methods for assessing the response to change in posture from supine to erect20,103,104: active standing (see section 4.2.2.1), head-up tilt (see section 4.2.2.2), and 24-h ambulatory BP monitoring (ABPM) (see section 4.2.3.4).
4.2.2.1 Active standing
Indications:
This test is used to diagnose different types of orthostatic intolerance (see Web Practical Instructions Web Table 1). A sphygmomanometer is adequate for routine clinical testing for classical OH and delayed OH because of its ubiquity and simplicity. Automatic arm-cuff devices, which are programmed to repeat and confirm measurements when discrepant values are recorded, are at a disadvantage due to the rapidly falling BP during OH. With a sphygmomanometer, more than four measurements per minute cannot be obtained without venous obstruction in the arm. When more frequent readings are required, as for initial OH, continuous beat-to-beat non-invasive BP measurement is needed.20,103,104
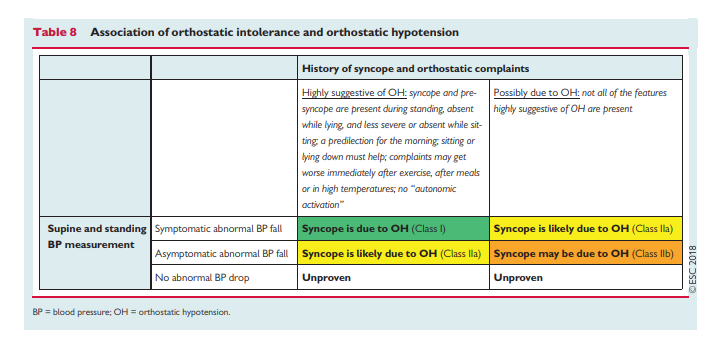
Diagnostic criteria: Abnormal BP fall is defined as a progressive and sustained fall in systolic BP from baseline value >_20 mmHg or diastolic BP >_10 mmHg, or a decrease in systolic BP to <90 mmHg. This definition of OH differs from the 2011 consensus6 in adding the 90 mmHg threshold. This Task Force believes that an absolute threshold of 90 mmHg of systolic BP is useful, especially in patients with a supine BP <110 mmHg. An isolated diastolic BP drop is very rare and its clinical relevance for OH diagnosis is limited. Orthostatic heart rate (HR) increase is blunted or absent [usually not >10 beats per minute (b.p.m.)] in patients with neurogenic OH, but increases or even exaggerates with anaemia or hypovolaemia. The probability that syncope and orthostatic complaints are due to OH can be assessed using the information given in Table 8.
4.2.2.2 Tilt testing
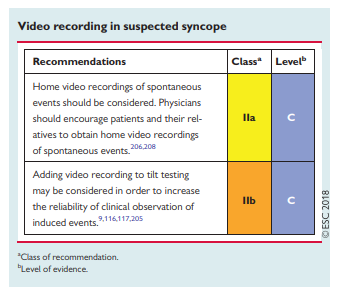
Since its introduction in 1986,105 many protocols have been reported with variations in the initial stabilization phase, duration, tilt angle, type of support, and pharmacological provocation. The most commonly used are the trinitroglycerin (TNG) test using 300–400 µg of sublingual TNG after a 20-min unmedicated phase,106,107 and the low-dose intravenous isoproterenol test, which uses incremental doses to increase average HR by about 20–25% over baseline (usually ≤3 µg/min).108,109 In a recent systematic literature review,110the overall positivity rate in patients with syncope was 66% for the TNG protocol and 61% for the isoproterenol protocol; the respective positivity rate in subjects without syncope (controls) ranged from 11–14%; and the test differentiated patients with syncope from controls with an odds ratio of 12. The methodology and classification of responses are described in section 6 of the Web Practical Instructions. Adding video recording to a tilt table permits objective and repeated review of clinical signs in relation to BP and HR, and helps to assess the relative contribution of bradycardia and hypotension to syncope (see section 5.2.6.3 and the explanatory video in Web Practical Instructions section 6.3.15), and to distinguish between VVS and PPS (see section 4.2.5).
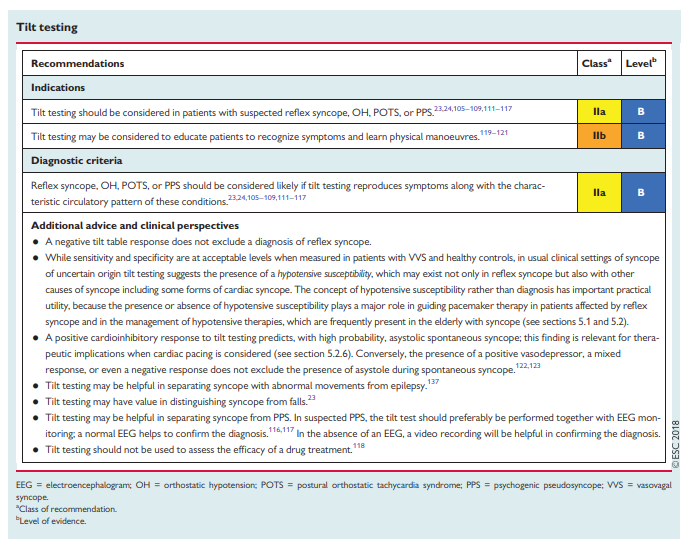
The clinical situation corresponding to tilt-induced syncope is that which is triggered by prolonged standing. The test should be considered: (i) to confirm a diagnosis of reflex syncope in patients in whom this diagnosis was suspected but not confirmed by initial evaluation105–109,111, and (ii) for the assessment of autonomic failure, especially for the reproduction of delayed OH (which could not be detected by active standing because of its delayed onset)23,24,112,113 and postural orthostatic tachycardia syndrome (POTS).114 Tilt testing may be helpful in separating syncope from PPS.115–117
Tilt testing has limited value in assessing treatment efficacy.118 However, tilt testing is widely accepted as a useful tool to demonstrate susceptibility of the patient to reflex syncope, especially a hypotensive (vasodepressive) tendency, and thereby to initiate treatment (e.g. physical manoeuvres, see section 5).119–121
The endpoint of tilt testing is the reproduction of symptoms along with the characteristic circulatory pattern of the indication mentioned above, namely the induction of reflex hypotension/bradycardia, OH, POTS, or PPS. The typical tilt test result patterns are shown in the Web Practical Instructions section 6.
Interpretation of tilt testing results in patients with reflex syncope:
Some studies122,123 compared the response to tilt testing with spontaneous syncope recorded by an implantable loop recorder (ILR). While a positive cardioinhibitory response to tilt testing predicts, with a high probability, an asystolic spontaneous syncope, the presence of a positive vasodepressor, mixed response, or even a negative response, does not exclude the presence of asystole during spontaneous syncope.122,123 [Emphasis added]
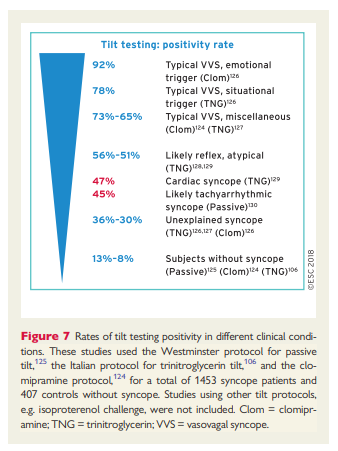
Tilt testing has an acceptable sensitivity124 and specificity106,124,125 when these are calculated in patients with true VVS or without a history of syncope. However, there is an inability to apply the test to populations with syncope of uncertain cause where it is hoped that tilt testing might prove decisive. In these clinical settings, tilt testing fails to deliver (Figure 7). Indeed, tilt testing was positive in 51–56% of patients with atypical clinical features suggesting a reflex mechanism,106,124–128 in 30–36% with unexplained syncope after full investigation,124,129 and in 45–47% with true cardiac arrhythmic syncope.130,131In other words, tilt testing offers little diagnostic value in patients for whom it is most needed. In these patients, a positive tilt test reveals a susceptibility to orthostatic stress.132 This hypotensive susceptibility plays a role in causing syncope irrespective of the aetiology and mechanism of syncope. For example, in arrhythmic syncope caused by paroxysmal atrial tachyarrhythmias, the mechanism is a combination of onset of the arrhythmia itself and hypotensive susceptibility, corroborated by positive tilt testing.130,131 Similarly, multifactorial mechanisms are likely in other types of cardiac syncope, e.g. aortic stenosis,133 hypertrophic cardiomyopathy (HCM),134 and sick sinus syndrome.135,136 The presence or absence of susceptibility explains the occurrence of syncope in some and not in others affected by the same severity of arrhythmia or structural defect. Tilt testing should now be considered a means of exposing a hypotensive tendency rather than being diagnostic of VVS. This concept has practical implications for therapy (see sections 5.1 and 5.2).
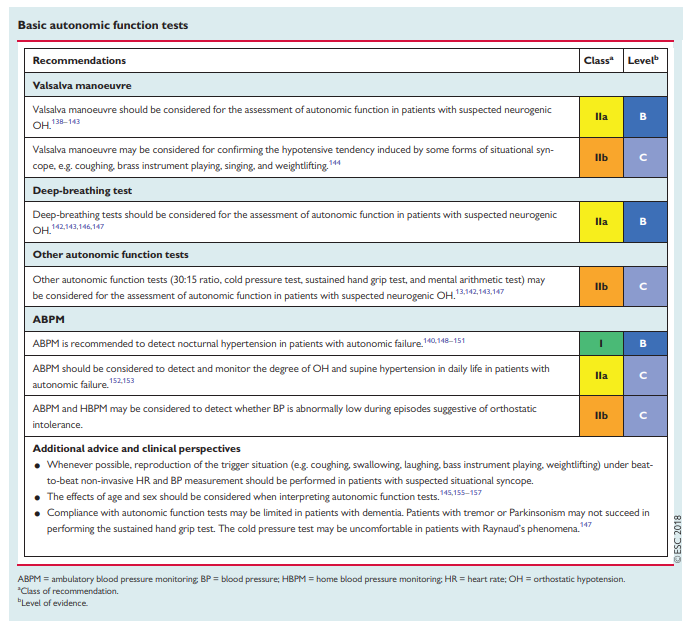
4.2.3 Basic autonomic function tests
Autonomic function assessment helps to identify autonomic failure as the underlying cause of syncope. [Unfortunately, for our patients, the publisher has chosen to place the Web Practical Instructions on performing these autonomic tests behind a firewall.]
4.2.3.1 Valsalva manoeuvr
The methodology of the Valsalva manoeuvre is described in section 7.1.1 of the Web Practical Instructions and in Web Video 2. There is strong evidence that the absence of a BP overshoot and an absence of a HR increase during the Valsalva is pathognomonic for neurogenic OH, occurring in primary and secondary autonomic failure, and the degree of hypotension and/or lack of compensation during forced expiration usually correlate with the degree of autonomic dysfunction and related symptoms.138–143 In contrast, a pronounced BP fall beyond what is normally expected during forced expiration, but a
normal chronotropic response during the manoeuvre, may occur in patients with suspected situational syncope, i.e. syncope occurring during some forms of situational syncope, e.g. coughing, brass instrument playing, singing, and weightlifting.1444.2.3.2 Deep breathing
The methodology of the deep-breathing test is described in section 7.1.2 of the Web Practical Instructions. Under physiological conditions, HR rises during inspiration and fallsduring expiration. HR variability during deep breathing (also called the expiratory/inspiratory index or E/I index) is >_15 b.p.m. in healthy individuals aged >50 years.145 There is strong consensus that blunted or abolished variation is suggestive of parasympathetic dysfunction.142,143,146,147
4.2.3.3 Other autonomic function tests
Further tests to evaluate cardiovascular sympathetic function include calculation of the 30:15 ratio, the cold pressure test, the sustained hand grip test, and mental arithmetic. There is weak evidence that these tests may be useful.13,142,143,147
4.2.3.4 Twenty-four-hour ambulatory and home blood pressure
monitoringTwenty-four-hour ABPM and home BP monitoring (HBPM) are
increasingly used to diagnose and monitor the treatment of hypertension.148 There is strong evidence that OH is frequently associated with a nocturnal ‘non-dipping’ or even ‘reverse-dipping’ BP pattern in patients with autonomic failure, with relevant therapeutic and prognostic implications140,148–151 (see Web Practical Instructions section 7.1.3). In these patients, ABPM allows the assessment of nocturnal hypertension, postprandial hypotension, and exercise- and drug-induced hypotension, as well as monitoring for side effects of antihypotensive regimens and pointing to additional disorders such as sleep apnoea.152 There is weak evidence that ABPM may also detect the degree of OH in daily life better than single office BP measurements.153HBPM may be used to investigate the cause of orthostatic intolerance, i.e. to clarify whether symptoms are due to OH or to other causes, such as vertigo or motor imbalance in Parkinson’s disease or multiple system atrophy. The evidence is weak. Finally, HBPM can be used to clarify that BP is not low during episodes of PPS.154
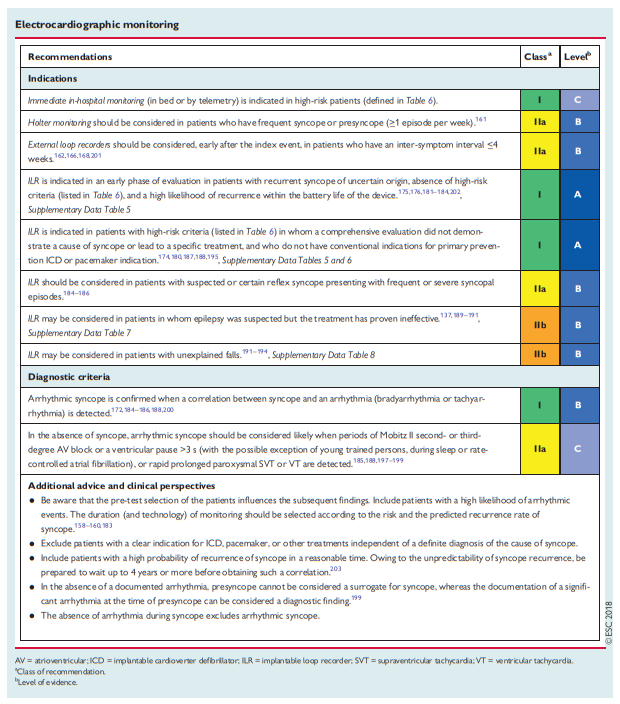
4.2.4 Electrocardiographic monitoring (non-invasive and invasive)
The role of ECG monitoring cannot be defined in isolation. As a rule, ECG monitoring is indicated only when there is a high pre-test probability of identifying an arrhythmia associated with syncope, such as those listed in Table 5.
4.2.4.8 Diagnostic criteria
The gold standard for the diagnosis of arrhythmic syncope is when there is a correlation between the symptoms and an ECG recording.195,196The presence of asymptomatic significant arrhythmias—defined as prolonged asystole (>_3 s), rapid supraventricular tachycardias (SVTs) (i.e. >160 b.p.m. for >32 beats), or ventricular tachycardias (VTs)—has been considered by several authors to be a diagnostic finding.185,188,197–199 On the other hand, although the absence of documentation of an arrhythmia during a syncopal episode cannot be considered to be a specific diagnosis, it allows the exclusion of an arrhythmia as the mechanism of the syncope. Most evidence in support of the above diagnostic criteria is indirectly based on the benefit of specific therapies guided by ECG monitoring in preventing
syncopal recurrences.172,184–186,188,200Even if the quality of evidence is moderate, there is strong consensus based on evidence from several controlled trials that acorrelation between symptoms and a documented arrhythmia, or the presence of some asymptomatic significant arrhythmias (defined above), is diagnostic of the cause of syncope and specific treatment must be prescribed.
The principal limitation of any ECG monitoring device is the
inability to record BP together with ECG. In reflex syncope, the
documentation of bradycardia/asystole during a syncopal episode does not rule out the possibility that a hidden hypotensive reflex is the principal cause for syncope, and that bradycardia/asystole is a secondary late event. This issue has important implications for therapy (see section 5). A classification of ECG recordings with their probable related pathophysiology is available in Web Table 6 and Web Practical Instructions section 8.
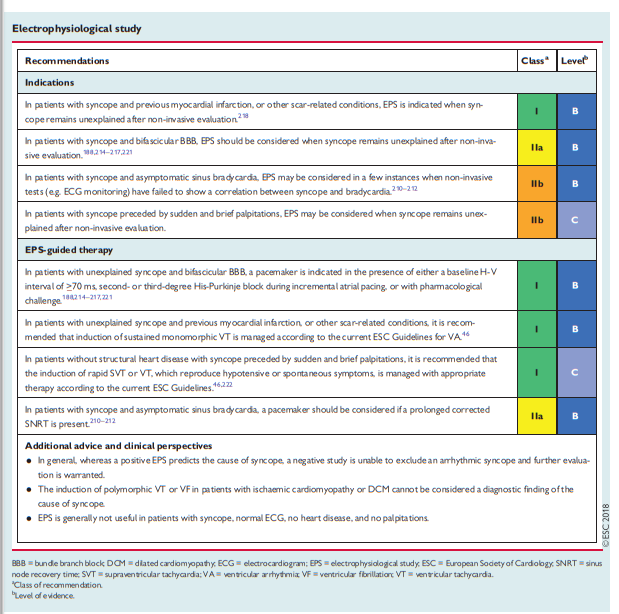
4.2.6 Electrophysiological study
Indications: In an overview of eight studies, including 625 patients with syncope undergoing EPS,209 positive results occurred predominantly in patients with structural heart disease. In recent years, the development of powerful non-invasive methods, i.e. prolonged ECG monitoring, showing a higher diagnostic value, has decreased the importance of EPS as a diagnostic test. In clinical practice, registry data show that approximately 3% of patients with unexplained syncope evaluated by cardiologists undergo EPS and even fewer if they are evaluated by other specialists.71 Nevertheless, EPS remains useful for diagnosis in the following specific clinical situations: asymptomatic sinus bradycardia (suspected sinus arrest causing syncope), bifascicular BBB (impending high-degree AV block), and suspected tachycardia.
4.2.7 Endogenous adenosine and other biomarkers
Established cardiac biomarkers such as troponin and B-type natriuretic peptide have been used to distinguish cardiac from non-cardiacsyncope and identify structural heart disease.223–225
[See 4.2.7.1 Adenosine (triphosphate) test and plasma concentration. See pp 27 and 28 of the PDF for details.]
4.2.8 Echocardiography
For patients with suspected heart disease, echocardiography serves to confirm or refute the suspicions in equal proportions and plays an important role in risk stratification.235,236 Echocardiography identifies the cause of syncope in very few patients when no more tests areneeded (i.e. severe aortic stenosis, obstructive cardiac tumours or thrombi, pericardial tamponade, or aortic dissection).237–239 In a literature
review, right and left atrial myxoma presented with syncope
in <20% of cases.240–2444.2.8.1 Exercise stress echocardiography
Upright or semi-supine exercise stress echocardiography to detect provocable left ventricular outflow tract obstruction should be considered in patients with HCM that complain of exertional or postural syncope, particularly when it recurs during similar circumstances (e.g. when rushing upstairs or straining). A gradient of >_50 mmHg is usually considered to be the threshold at which left ventricular outflow tract obstruction becomes haemodynamically important.245–249
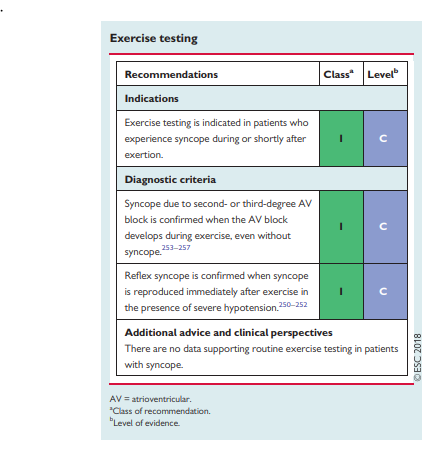
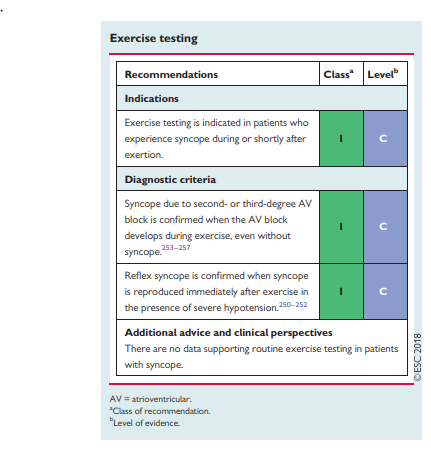
4.2.9 Exercise stress testing
Exercise-induced syncope is infrequent, and the literature is limited to case reports. Exercise testing should be performed in
patients who have experienced episodes of syncope during or
shortly after exertion. Syncope can occur during or immediately
after exercise. These two situations should be considered separately. Indeed, syncope occurring during exercise is likely due to cardiac causes (even though some case reports have shown that it might be a manifestation of an exaggerated reflex vasodilatation), whereas syncope occurring after exercise is almost invariably due to a reflex mechanism.250–252 Tachycardia-related exercise induced
second- and third-degree AV block has been shown to be located distal to the AV node253 and predicts progression to permanent
AV block.254,255 A resting ECG frequently shows intraventricular conduction abnormalities,253,254 but cases with a normal resting ECG have also been described.256,257 There are no data supporting an indication for exercise testing in a general population with syncope.
4.2.10 Coronary angiography
In patients presenting with syncope and obstructive coronary artery disease, percutaneous coronary intervention is not associated with a significant reduction in readmission for syncope.258 Angiography alone is not diagnostic of the cause of syncope. Therefore, cardiac catheterization techniques should be carried out in suspected myocardial ischaemia or infarction with the same indications as for patients without syncope.






This is the end of my post on “The Evaluation Of Syncope In Primary Care – Help From The “2018 ESC Guidelines for the diagnosis and management of syncope”.
For the treatment of syncope please see my post “The Treatment Of Syncope In Primary Care – Help From The ‘2018 ESC Guidelines for the diagnosis and management of syncope’”. Resource (5) below.
Resources:
(1) 2018 ESC Guidelines for the diagnosis and management of syncope [PubMed Citation] [Full Text HTML] [Access the Full Text PDF from the Full Text HTML link]. Eur Heart J. 2018 Mar 19. doi: 10.1093/eurheartj/ehy037. [Epub ahead of print]
(2) Practical Instructions for the 2018 ESC Guidelines for the diagnosis and management of syncope [PubMed Citration] . Eur Heart J. 2018 Mar 19. doi: 10.1093/eurheartj/ehy071.
(3) Practical Instructions for the 2018 ESC Syncope Guidelines [a summary of the above article from the American College of Cardiology]. Apr 04, 2018 | Debabrata Mukherjee, MD, FACC.
(4) 2018 ESC Guidelines for the diagnosis and management of syncope – Supplementary Data [Full Text PDF]. European Heart Journal (2018) 00, 1–12 doi:10.1093/eurheartj/ehy037.
(5) The Treatment Of Syncope In Primary Care – Help From The “2018 ESC Guidelines for the diagnosis and management of syncope” Posted on May 6, 2018 by Tom Wade MD.



