Because this blog is simply my peripheral brain, these are simply my study notes on the topic.
Dr. Weingart of EMCrit (in EMCrit 207 – A Case to Acid Test your Resus Logistics
September 5, 2017) reviews the management of a 52 year old hypotensive female with end stage renal disease who comes into his department by BLS ambulance (she was too sick to wait for paramedic ambulance).
The podcast is only 27 minutes long with wonderful examples of clinical reasoning guiding management.
Before or after listening to the podcast be sure and review the links in the show notes:
Items of Interest
- Dirty Double
- In this post Dr. Farkas recommends simultaneous placement of a femoral venous catheter and femoral arterial catheter in the hemodynamically unstable patient – optimally with ultrasound guidance.
- Push-Dose Pressor Update
- In this podcast Dr. Weingart reviews when and why to use a push dose pressor. If you type “push dose pressor” into the search box of my blog, you will get a list of eleven posts linking to emergency medicine experts’ advice on the use of push dose pressors.
- RUSH Exam
- In this podcast and shownotes Dr. Weingart goes over the Rapid Ultrasound Exam in Shock and Hypotension (RUSH).
- On my blog there are a 79 posts (usually with links to videos) about all aspects of bedside ultrasound. See the category “Ultrasound Imaging” for the complete list.
- Hyperkalemia Podcast 32
- The following learning points are from #32:
- Learning Points:
1. When a patient is bradycardic, especially if irregular, one must always think of hyperK and one must get a 12-lead ECG.
2. One must recognize this pattern as hyperK
3. Calcium’s effect is almost miraculous
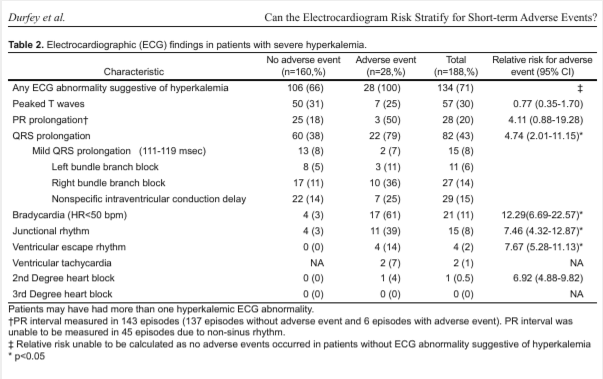
4. Slow atrial fibrillation implies an sick AV node, or one affected by electrolytes, ischemia, or medications/drugs. Otherwise, the ventricular response should be fast.- In the shownotes of podcast 32 Dr. Weingart from 2010, Dr. Weingart updates with a link to this 2017 article – Severe Hyperkalemia: Can the Electrocardiogram Risk Stratify For Short Term Adverse Events? – The article concludes that the answer is yes. I’ve included Table 2 from the article in Additional Resources below.
- HOP Killers
- Hypotension (or the potential for hypotension), Oxygenation Problems (or the potential for hypoxia), and PH Problems (Acidosis that requires compensatory hyperventilation)
- These are the patient characteristics that can cause intubation and positive pressure ventilation to lead to cardiovascular collapse.
- See my post The Phsiologically Difficult Intubation – Critical Help From Drs. Weingart and Mellick Posted on September 1, 2016 for links to these teachers’ posts on how to mitigate the HOP killers.
- Peripheral Vasopressors Podcast 105
- Another must listen to with tons of practical tips and references.
- SLED
- Slow Low Efficiency Dialysis (SLED). I couldn’t find this lecture on the Intensive Care Network (ICN)
- So here is a link to IHD vs CRRT vs SLED from Life In The Fast Lane.
- And a link to the PDF Sustained Low Efficient Dialysis: A New Look at Renal Replacement Therapy from the The Ottowa Hospital ICU.
Additional Resources:
(1) Table 2 from Severe Hyperkalemia: Can the Electrocardiogram Risk Stratify For Short Term Adverse Events? West J Emerg Med. 2017 Aug;18(5):963-971. doi: 10.5811/westjem.2017.6.33033. Epub 2017 Jul 10.: