Today, I review, link to, and excerpt from 2oo A retrospective analysis of triple rule-out CT coronary angiography (TRO-CTA) from a secondary care hospital in the United Kingdom [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Lewis G, Lagan J, Ruzsics B200 A retrospective analysis of triple rule-out CT coronary angiography (TRO-CTA) from a secondary care hospital in the United KingdomHeart 2024;110:A210-A211.
All that follows is from the above resource.
Abstract
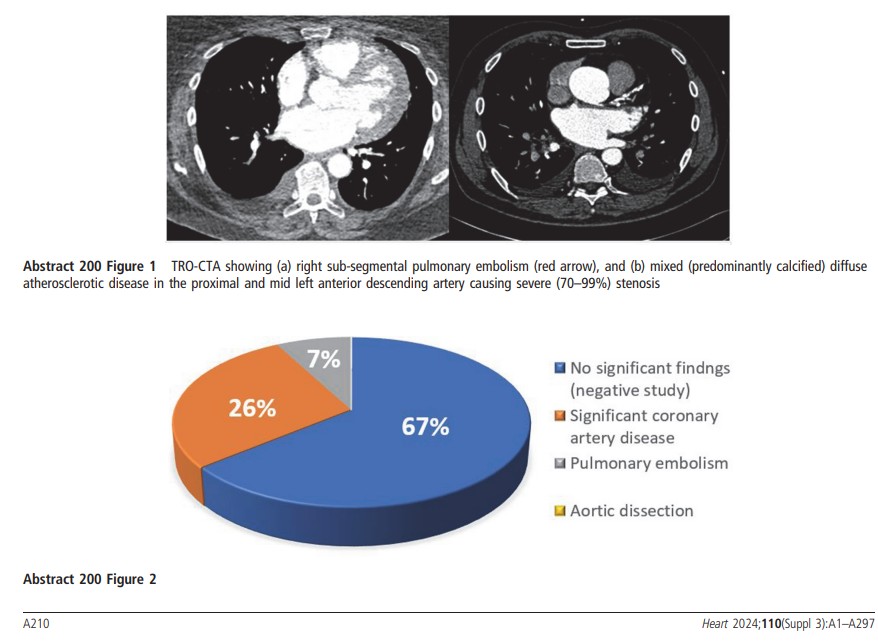
Introduction Triple rule-out (TRO) computed tomography angiography (CTA) can provide a cost-effective assessment of the coronary arteries, pulmonary arteries, and aorta in appropriately selected patients with acute chest pain and wide differential diagnosis (figure 1). Limited experience is described in the literature on use within the United Kingdom (UK) healthcare system.
Methods Retrospective analysis of consecutive patients undergoing dedicated TRO-CTA between 1st January 2015 and 1st April 2023 in a large UK teaching hospital. With limited local provision and accessibility, TRO-CTA was requested at the discretion of the reviewing cardiologist if deemed appropriate.
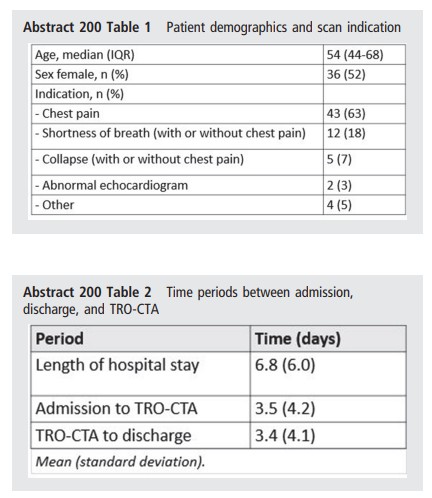
Results In total, 68 patients underwent dedicated TRO-CTA (table 1). TRO-CTA diagnosed significant coronary artery disease (CAD) in 18 (26%) patients and acute pulmonary embolism (PE) in 5 (7%) patients. No cases of aortic dissection were identified, and no significant findings were seen in 45 (66%) of patients (figure 2). D-dimer and high-sensitivity troponin T were performed in 41 (60%) and 61 (90%) patients; neither biomarker associated with PE (p=0.94) or significant CAD (p=0.22) respectively. Protocols used prospective (64%), retrospective (13%) and high-pitched spiral (22%) acquisition with radiation use was significantly reduced with high-pitched spiral compared to prospective (mean DLP 819 vs 237 mGycm, p < 0.001). Mean length of stay was 6.8 days with a mean time from admission to TRO-CTA of 3.5 days (table 2).
Conclusions TRO-CTA provided a high diagnostic yield in highly selected patients and eliminated the need for additional testing in approximately two-thirds of patients. Introduction of formal inclusion criteria and expanding capacity may contribute to reduce the length of hospital stay.