Today I review a series of posts on IV Pressors In The Treatment Of Life-Threatening Hypotension. Here are links to the posts and brief summaries.
Outstanding YouTube Video: “Push Dose Pressors for EMS: Epinephrine and Norepinephrine”
Posted on November 17, 2023 by Tom Wade MDToday’s resource is an outstanding brief resource (16:31). The best way to rapid review is to read the auto-generated transcript (so you’ll need to double check that the computer hasn’t made any mistakes). To view the transcript, watch the video on YouTube and follow along on the transcript.
Today, I reviewed and embedded the excellent YouTube video, Push Dose Pressors for EMS: Epinephrine and Norepinephrine.
Mar 9, 2022Sometimes a small dose of epinephrine or norepinephrine can keep a patient from becoming hypotensive during intubation, or may help bridge the patient to a continuous infusion. Dr. Pickett talks about simple methods for mixing and administering push doses of these pressors and how to administer the infusion. NOTE: It is ASSUMED you already know the indications, contraindications, and side effects of these drugs. This video is NOT a comprehensive review of these medications.
Making a push dose epinephrine syringe:
Take a 1:10,000 cardiac epi syringe (1 mg of epinephrine in 10 cc). We’re not going to push this because this is way too much.
This syringe has 1 mg of epinephrine in 10 ml of saline which is 0.1 mg per ml.
Again, the above concentration is way too high to use as a push dose pressor. And badness could happen (like a fatal arrythmia).
So, I’m going to waste 9 cc of the syringe so there is only one cc in the syringe. The concentration is in the syrine is still 0.1 mg per 1 ml, just like it was when there was 10 ml in the syringe. The concentration hasn’t changed yet; we’re about to do that.
I’m going to draw out 9 ml of saline from the bag into the syringe with the one ml of epinephrine, 0.1 mg/ml.
I will draw [up 9 cc of normal saline into the syringe] and now I’ve got 10 cc’s again.
So my concentration in that syringe right there [now] 0.1 milligrams in 10 ml.
So it is [now] .01 milligrams or 10 micrograms per ml 10
mics per ml epinephrine.Summary Slide:
So now when i push this mixture . . .I’m going to push 2 ml at a time that will give me 20 micrograms or 0.02 milligrams of epinephrine.That’s enough to kind of bump that pressure for just a fewparalytics and so forth or it gets me a chance to mix up whatever infusion of a presser that i’m going to use. . .We are currently[at the time of this podcast] running out of cardiac epinephrine syringes, 1 mg in 10 ml. So Dr. Pickett gives us an a simpler alternative way to make up a push dose epi syringe, especially when we’re going to start an epinephrine infusion.
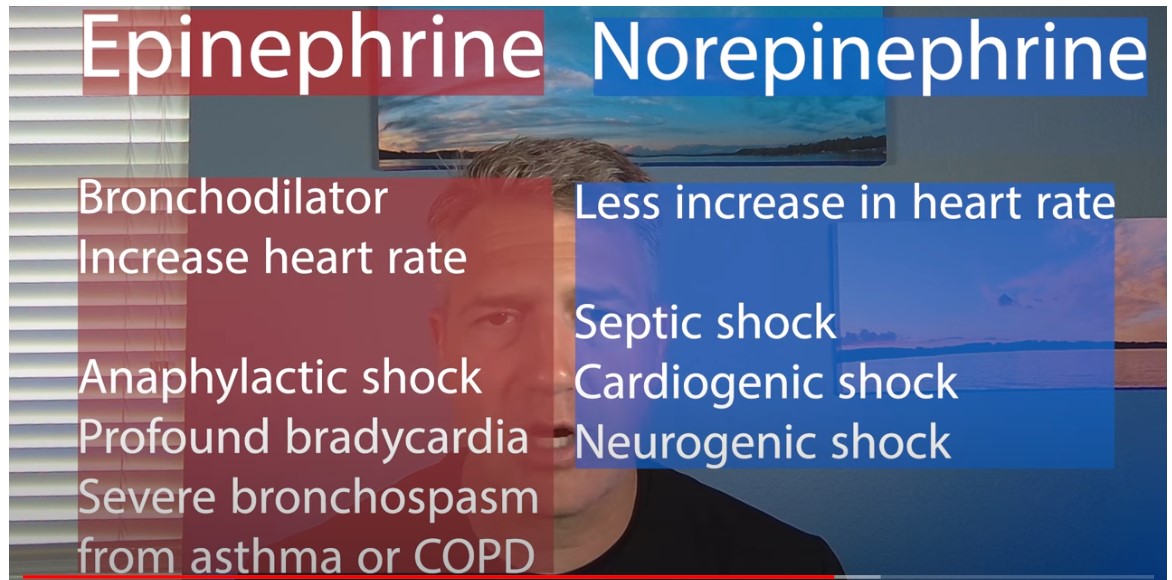
When do I like [an] epinephrine infusion? Couple reasons: one, anaphylaxis. Epinephrine is the drug [for that] and I like the intramuscular epinephrine but that to me is a bridge to get themIt’s going there right away and that’ why I like it. So if you’ve got somebody with good anaphylaxis going on, then, yeah, go ahead give them the IM epinephrine but then start an epinephrine infusion.
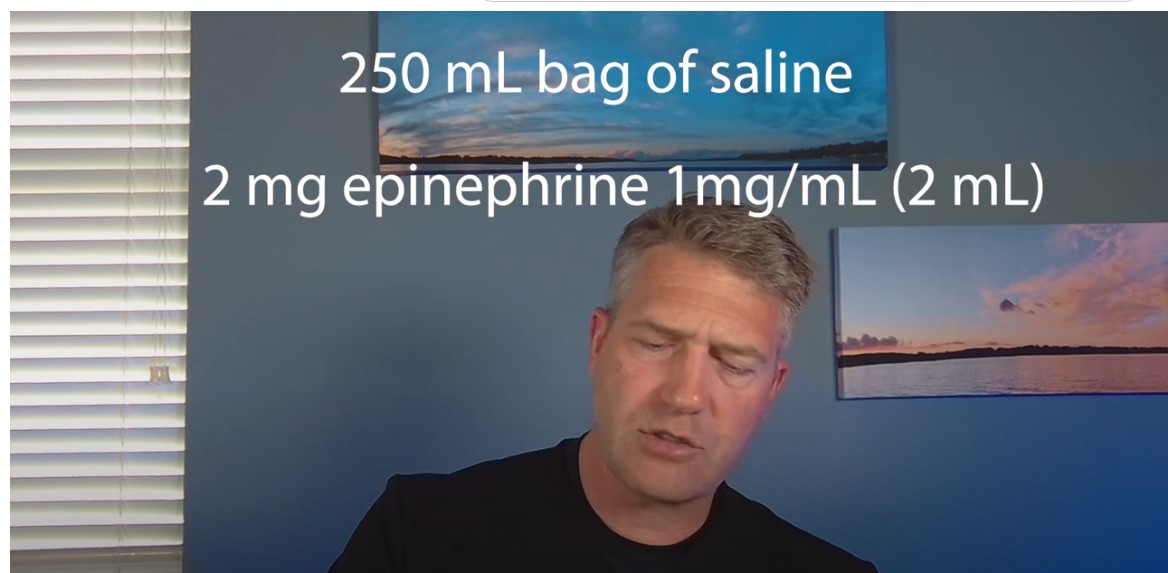
So, I want to make a an epinephrine infusion. So I’m going to take a 250 ml bag of, in this case saline 0.9 sodium chloride.
And I’m going to grab two of these little guys–this is epinephrine one milligram in [a] one ml [vial] (so the same thing you’re going t0 draw up for your for your intramuscular dose, right).
So I’ll grab two of those [vials] and we’ll do the medication crosscheck. . . .
So i’m going to draw that up and here so i’ve got some already drawn up
I’ve got 2 mls of epinephrine 1 to one thousand or one milligram [per] one ml so there’s two milligrams of epinephrine in here [in my syringe].
Well now I take my trusty 250 ml of fluid and I’m going to inject that [syringe of 2mg 0f epinephrine in 2ml] right in there, so again through the medication port.
9:41 Boom, injecting that two milligrams in here.
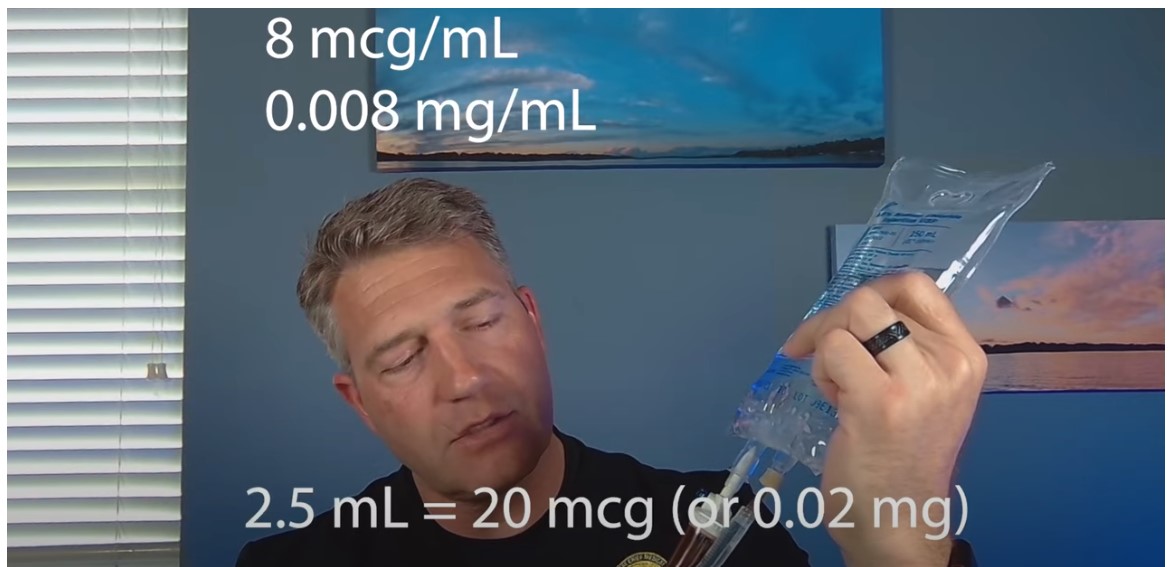
And now so mix that up. Okay we’re not like shaking it vigorously we don’t make a whole bunch of bubbles. We don’t make like foam in there. We’re just, you know, inverting it, making sure that it gets mixed around.
9:56My concentration in this bag now is eight micrograms per ml (so eight mics per ml.)Now remember what was the dose for push-dose epinephrine? Oh, yeah, 20 micrograms.So if I draw up now from this bag, two and a half mls [into a syringe], [I’ve] got two and a half ml’s right there [in the syringe].That’s 20 micrograms of epinephrine, so that’s my push dose. . . . Give them a little push dose and start running the infusion. And so that gives them that loading dose brings that pressure up.
And then we can maintain that [pressure] with the continuous infusion of epinephrine.
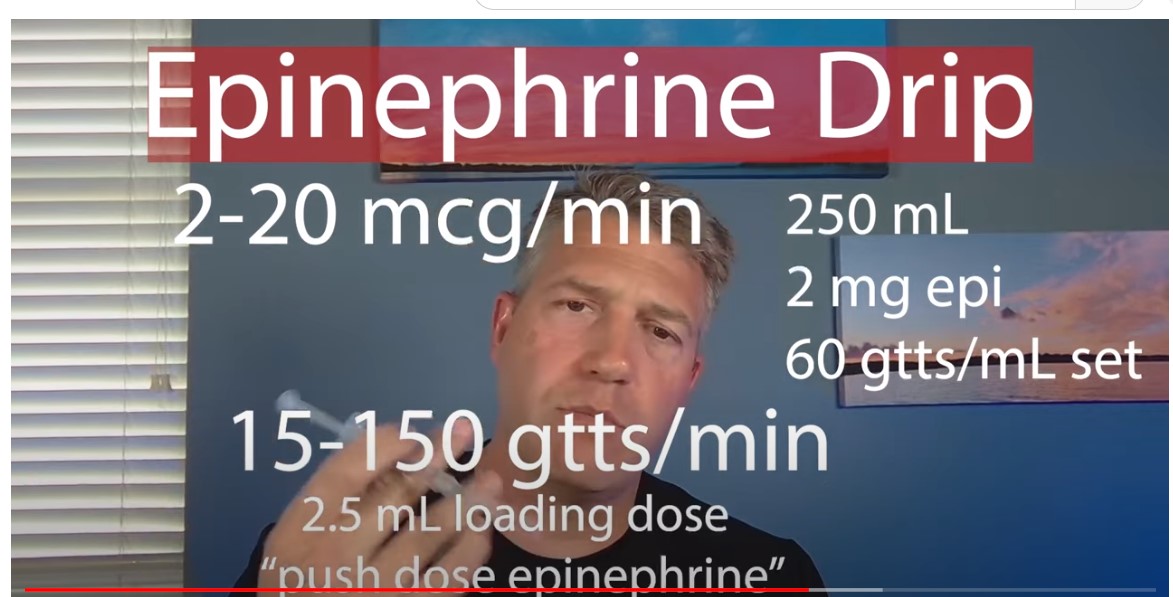
What dose am I going to continue this [this continuous dose epinephrine] on?So we want to go 2 to 20 micrograms per minute [for our constant infusion].10:40
So if i have this 250 ml bag of my epinephrine solution hannging] and I’ve got this on a 60 drop per ml set (so a micro drip set if you will), then it is 15 to 150 drops per minute for that 2 to 20 micrograms per minute–
So one drop every four seconds up to 150 drops per minute so. It’s like two and a half drops per second
11:07
So you can just titrate that up and down as you need to.
Now that’s approximate, okay. Like these aren’t that precise instrument. but that’ll get you where you need to be.
11:18
So again it’s 2 to 20 mics per minute, 15 to 150 drops per minute, is your dose when running the infusion
Two and a half cc’s gets you your bump to bring their pressure up to give them that loading dose.
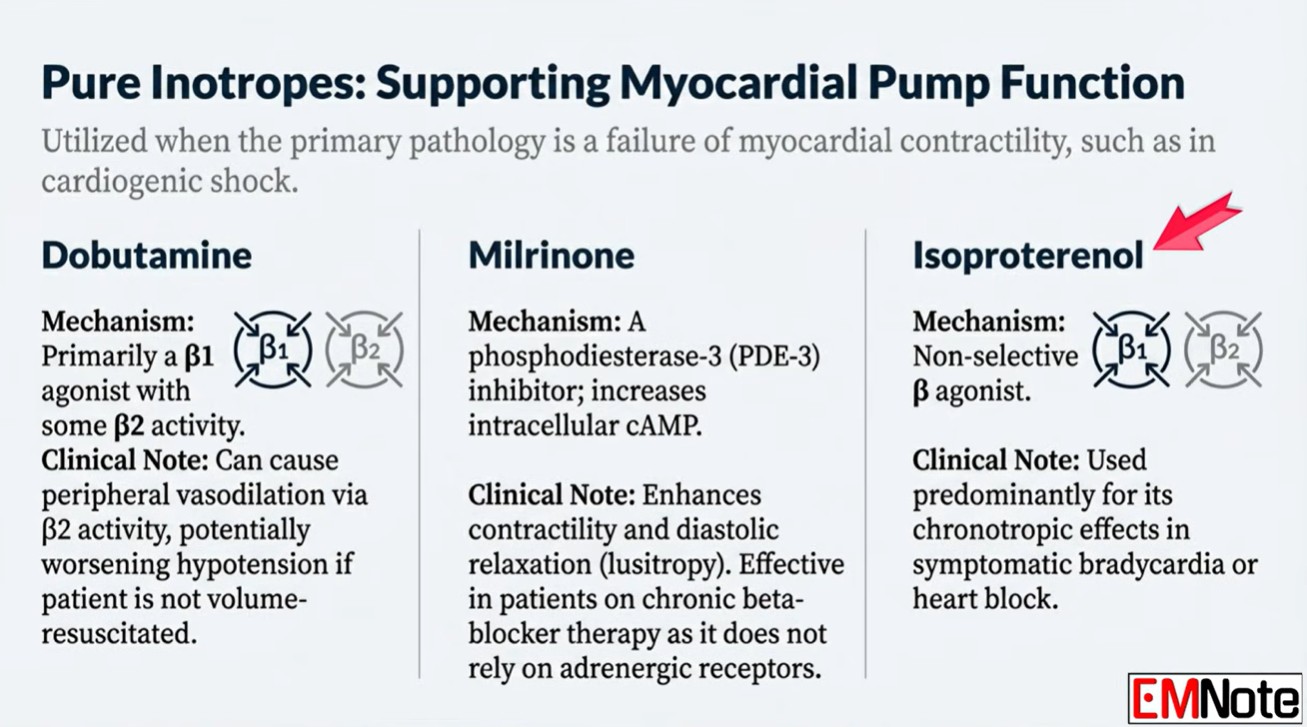
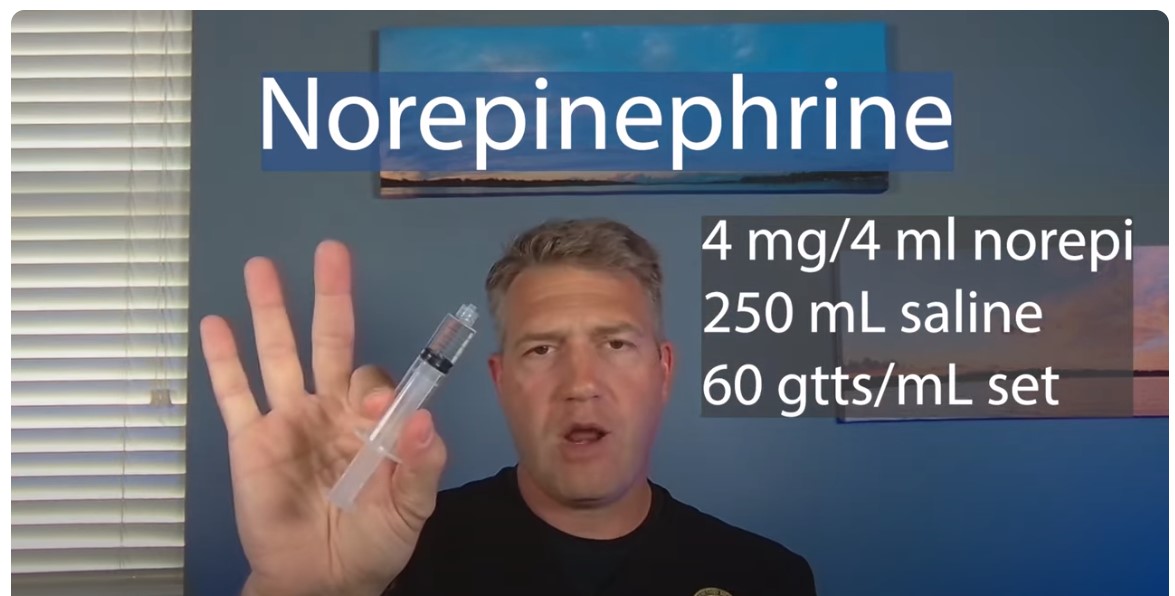
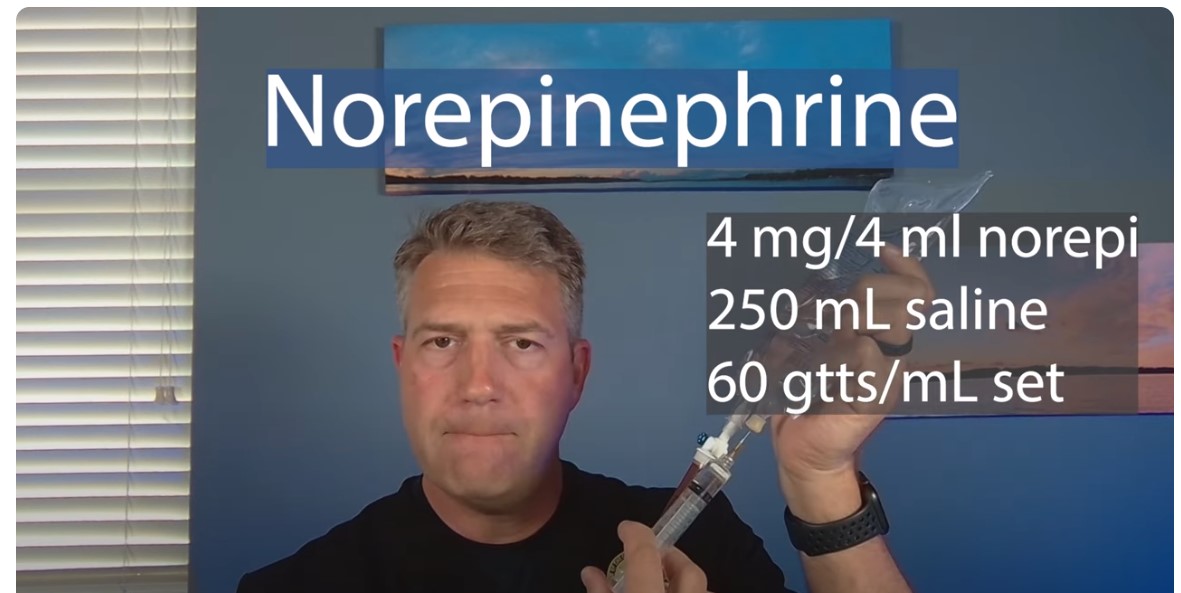
Obviously, we’re not going to treat hemorrhagic shock with a pressor, but others (spinal shock, neurogenic shock,cardiogenicshock, septic shock)–those things we will treat with norepinephrine preferentially.11:5111:55So here’s how we do this
11:58I get out my norepi. I’ve got four mls (four milligrams) norepinephrineright here. I’ll pop that and draw that up.
And now i have four mls right here of norepinephrine again i’m going to taket hat 4 mls
and i’m going to put it in a 250 cc bag 9250 ml bag) of saline.
I’m just going to pop this in here like so.
Boom, four ml’s in there. [Invert the bag back and forth to mix the solution. Don’t shake it as we don’t want bubbles in the solution.]
What’s my concentration here?Now okay it is 16 micrograms per ml in here.So what is my push dose for norepinephrine?Usually it’s around 20 to 30 micrograms.So if I draw up 2 mls of this [it will be 32 micrograms]So this will be close enough. 2 mls will get you 32 micrograms of this.
And that 2ml that’s that’s your push dose right there.
So you give them that 2ml bump and then you can start the drip.
If you are just doing it because you’re
gonna rsi somebody and they’re just kind of, you know, tenuous blood pressure but they’re not to the point where you want
to start them on a presser just yet, then okay mix this up drop your 2 mls push that as your push dose presser before you push the paralytics and the and the sedatives.
And then if you need it you’ve got it [the infusion bag].
It’s already made because this is the concentration that we’re going to use for running an infusion. so what’s our dose for an infusion for norepinephrine?
[It] is 2 to 12 micrograms per minute. So with at this concentration right here
it’s between 8 and 45 drops per minute so a little bit tighter range than what we have with the epinephrine.
But that will get you where you need to be.
Again that’s on a 60 drop micro drip set.






How To Effectively Use Vasopressors – Posts From Dr. Farkas And Podcasts From Dr. Weingart
Posted on June 23, 2018 by Tom Wade MDBecause I have mostly practiced in critical access hospitals, my focus has always been how can we keep the critically ill patient alive and potentially salvageable until the helicopter arrives.
And the immediate appropriate treatment of shock is an important topic for clinicians working in critical access hospitals.
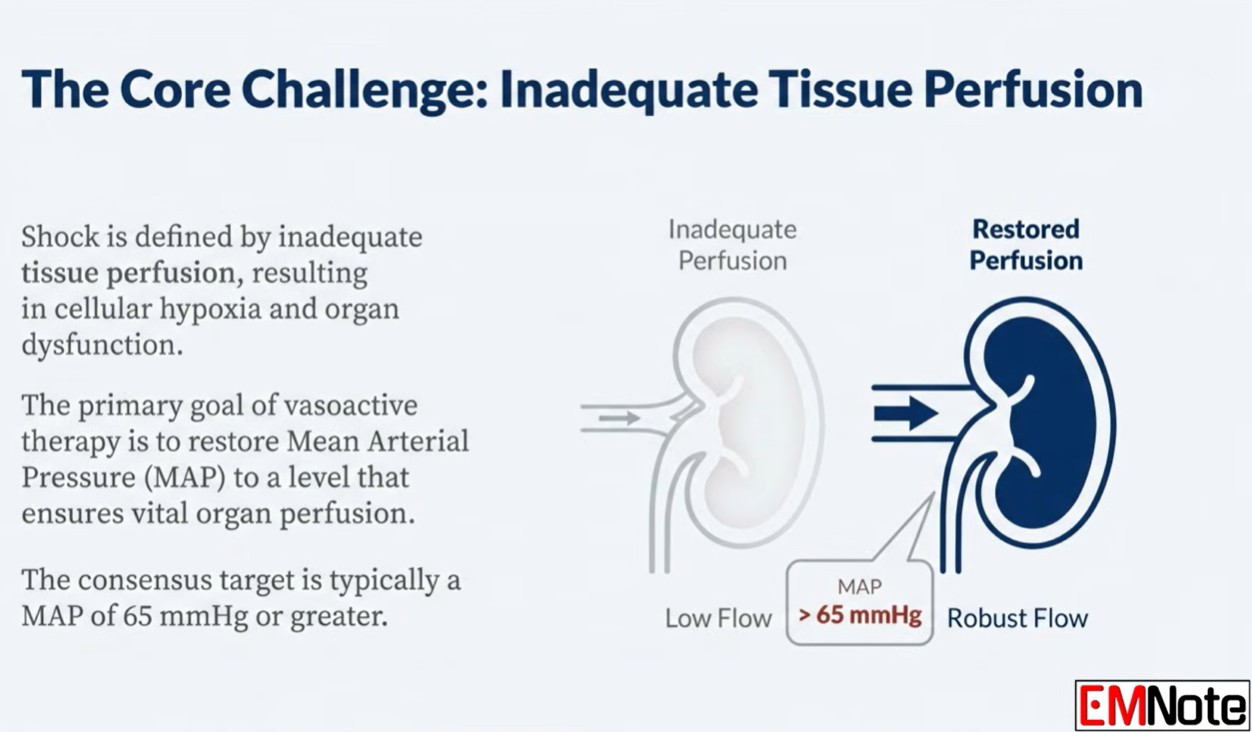
It is critical to defend the Mean Arterial Pressure (MAP). Do something immediately (meaning vasopressors) when the MAP goes low while you figure out the cause of the problem and treat it.*
*See Resource (4) EMCrit 201 – Deeper on Vasopressors and Athos 3 with Mink Chawla
June 12, 2017 by Scott WeingartSo first I’ll review (1) PulmCrit- Epinephrine challenge in sepsis: An empiric approach to catecholamines April 25, 2016 by Dr. Josh Farkas, which has an outstanding approach to the use of vasopressors. I’ve reviewed this post before in Practical Vasopressors And More In Septic Shock – Help From Drs. Farkas, Weingart, and Others Posted on June 17, 2017 by Tom Wade MD but it fits with (2) so I’ll review it again.
Then I’ll review (2) PulmCrit- High dose vasopressors: Never surrender
June 4, 2018 by Josh FarkasAnd finally I’ll link to Dr. Weingart’s podcast (3) Podcast 87 – Mind of the Resuscitationist: Stop Points November 26, 2012.
As always these extracts are my study notes to help fix Dr. Farkas’ posts in my mind.
Here are extracts from (1) PulmCrit- Epinephrine challenge in sepsis: An empiric approach to catecholamines April 25, 2016 by Dr. Josh Farkas [but review the entire post – note to myself]:
Introductory case
A 55-year-old woman was admitted with toxic shock syndrome. Her norepinephrine requirement was labile, fluctuating between 15 mcg/min and 30 mcg/min. Bedside echocardiogram showed a dilated inferior vena cava without respiratory variability, and a normal ejection fraction. On examination her extremities were cool and her urine output was marginal.Epinephrine 4 mcg/min was added, with an improvement in blood pressure, perfusion, and urine output. She reported feeling better, and over the next hour the norepinephrine was weaned off. Her lactate increased from 2 mM to 6 mM. The ICU team was pleased with this epinephrine-induced rise in lactate, a positive prognostic sign. Sure enough, she continued to improve and was weaned off vasopressors entirely over the next 18 hours.
Foundational concept #1: Vasopressors don’t always behave according to the textbook.
Individual patients vary considerably in how they respond to vasopressors. Two factors in particular may contribute to this variability.
Endogenous sympathetic response
Variable end-organ sensitivity
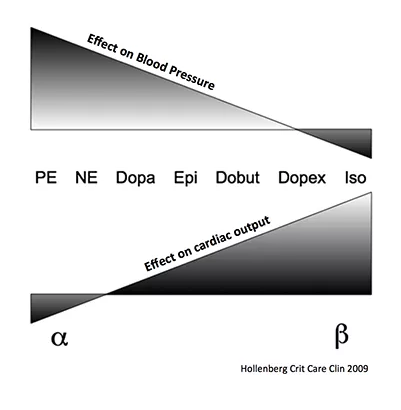
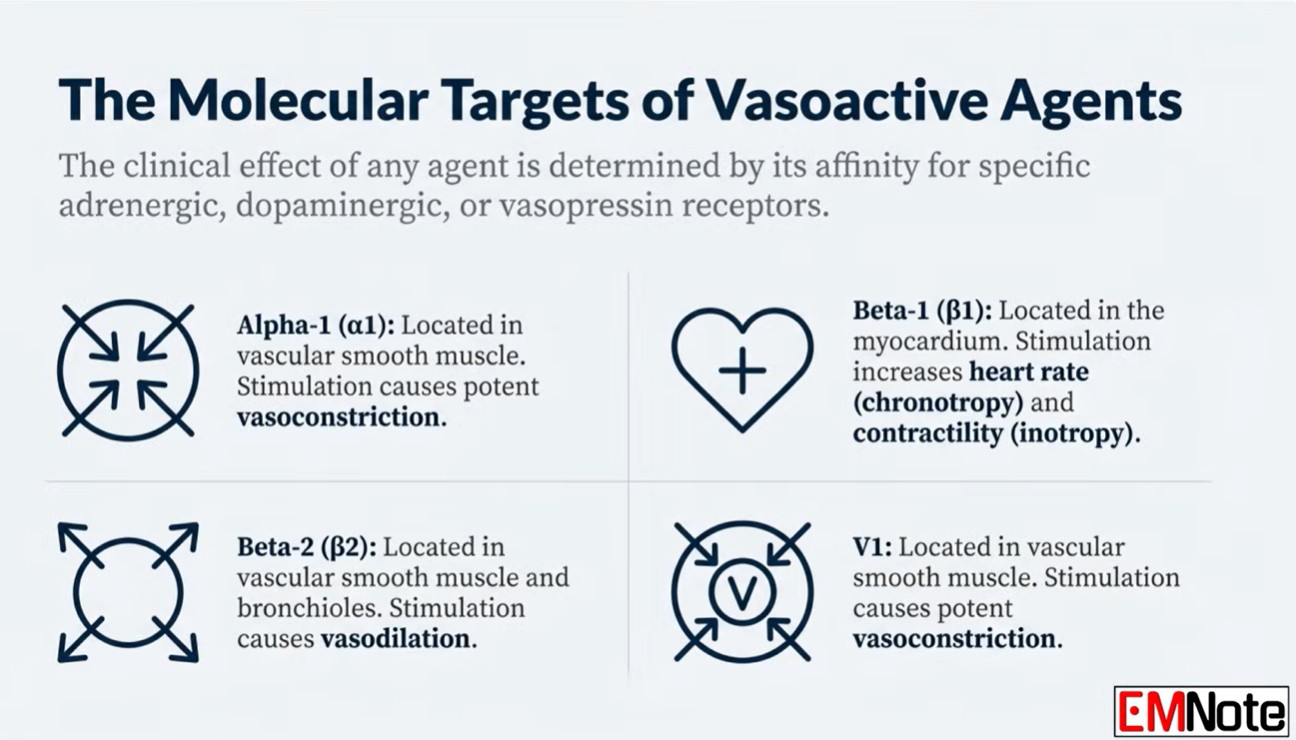
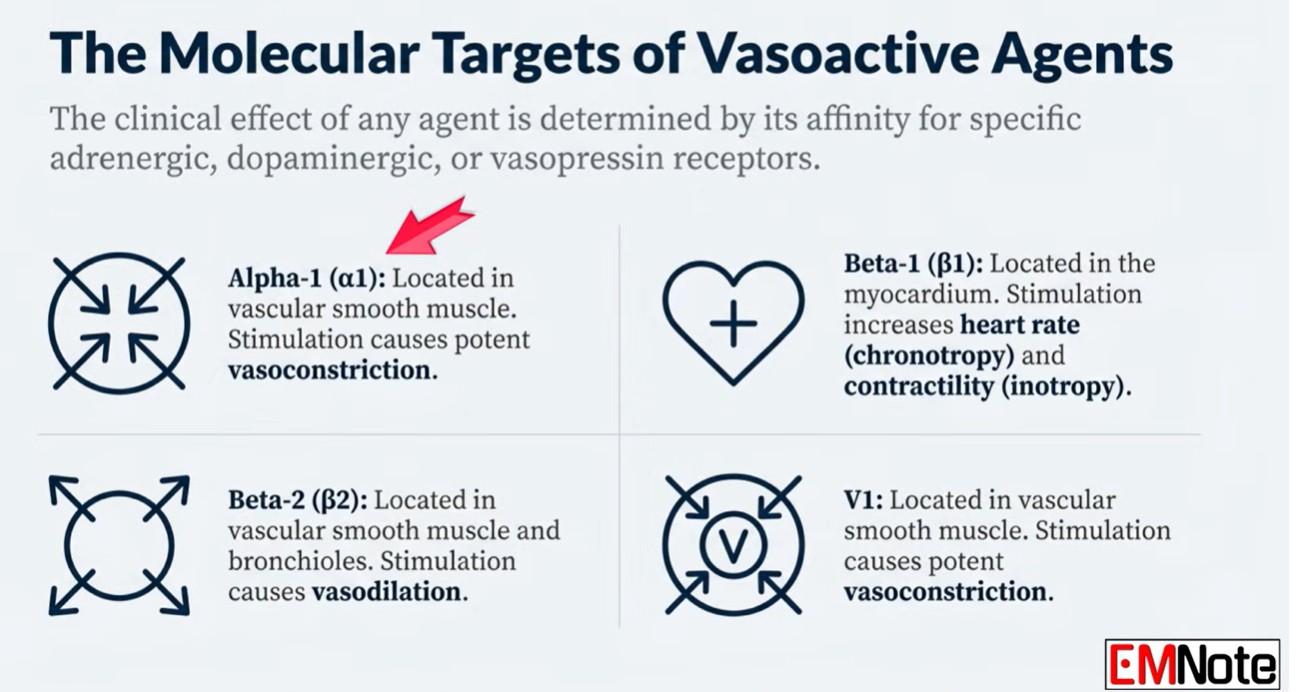
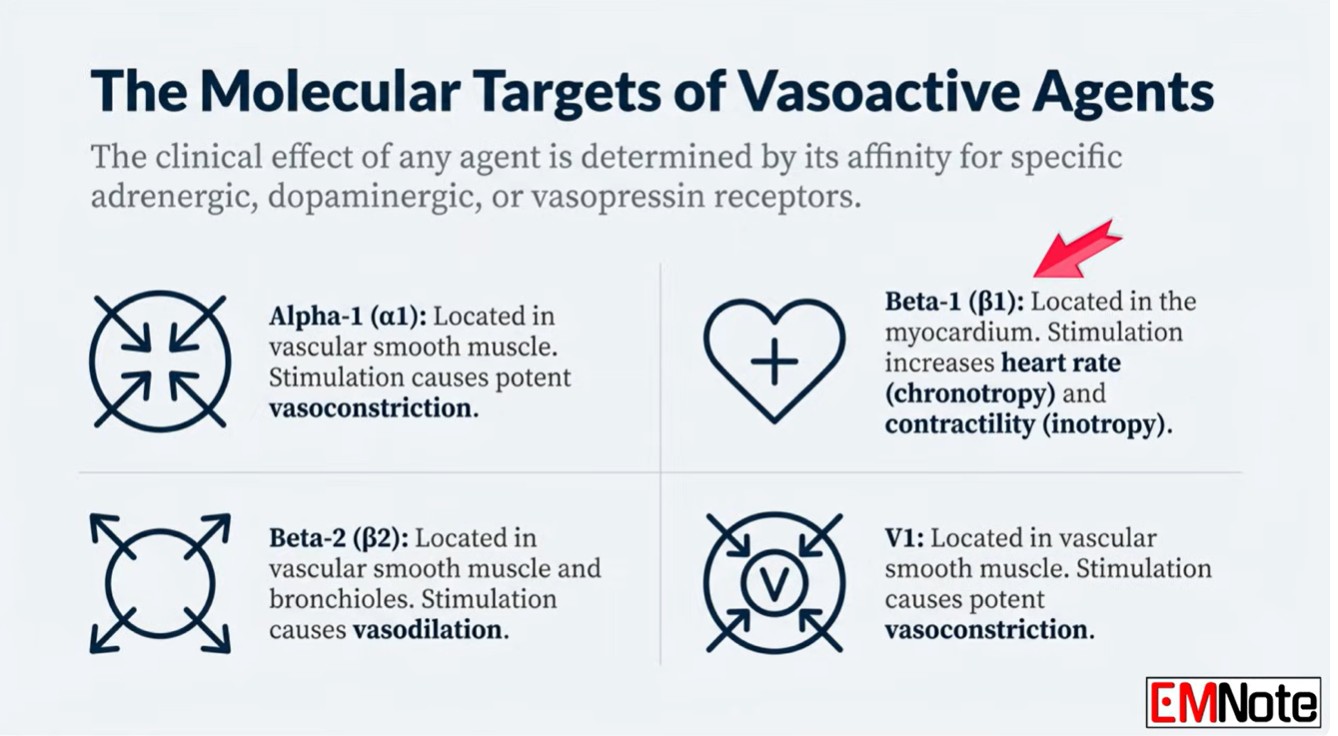
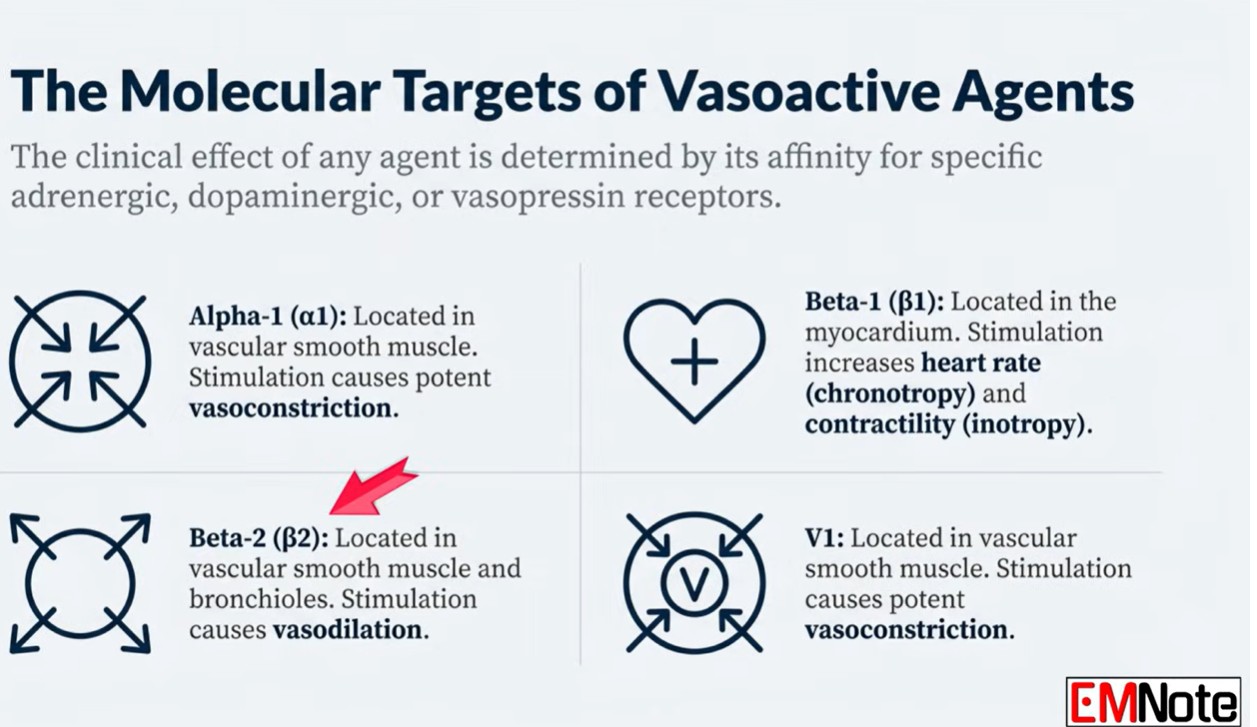
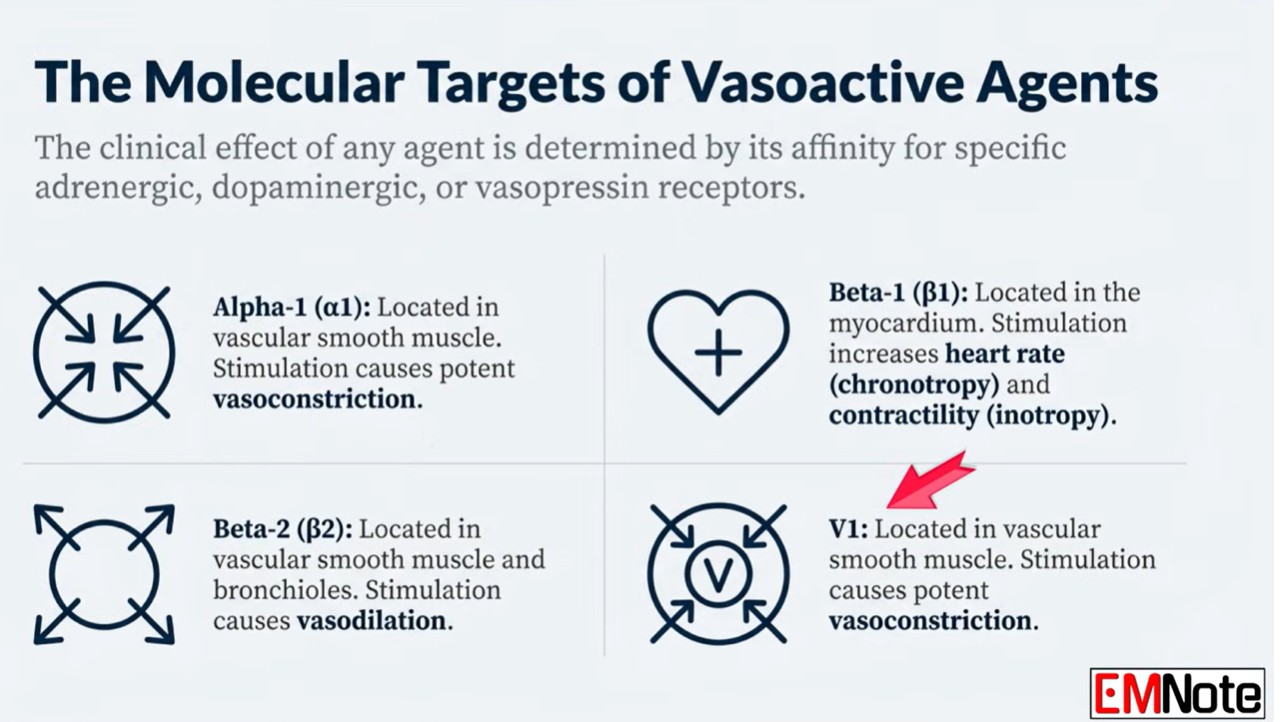
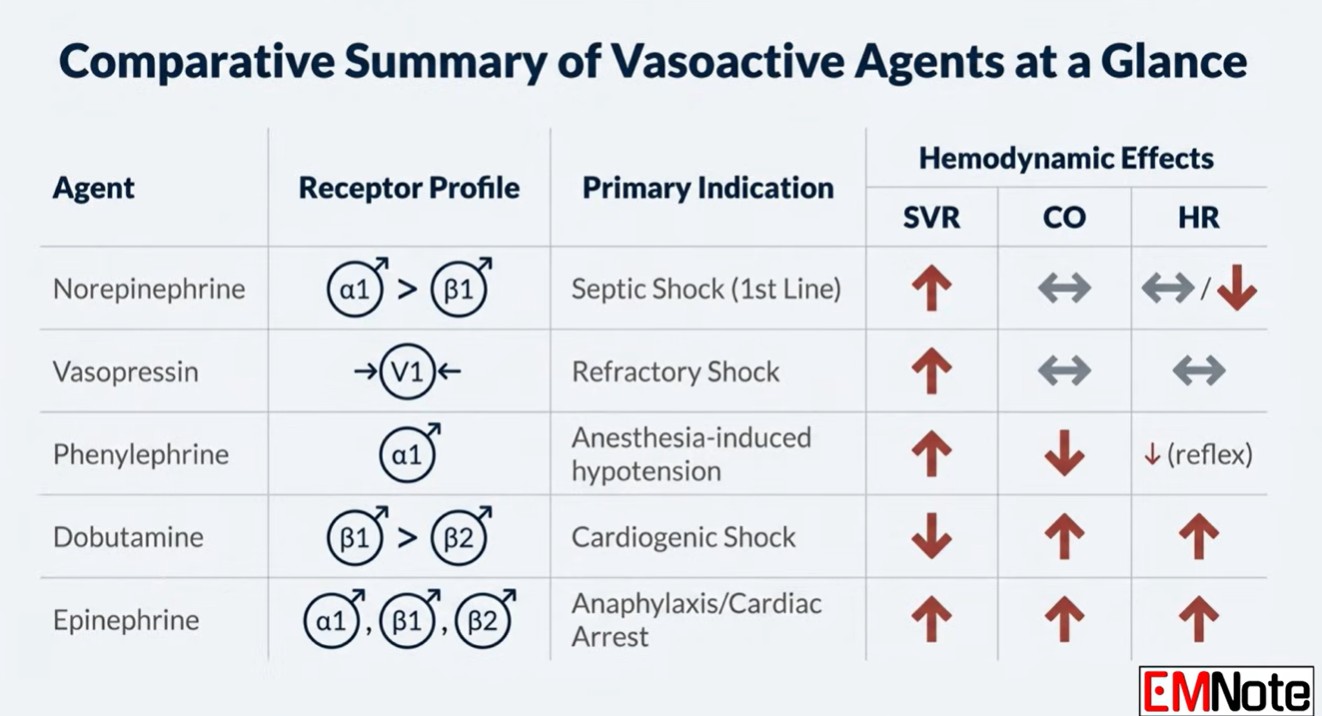
The differences between various catecholamines results from the ratio of stimulation of alpha-receptors vs. beta-receptors (figure below). However, patients vary in the responsiveness of their heart and vasculature. For example, reduced cardiac sensitivity to beta-agonists is common in advanced sepsis, due to receptor down-regulation. Refractory vasodilation is also well described.
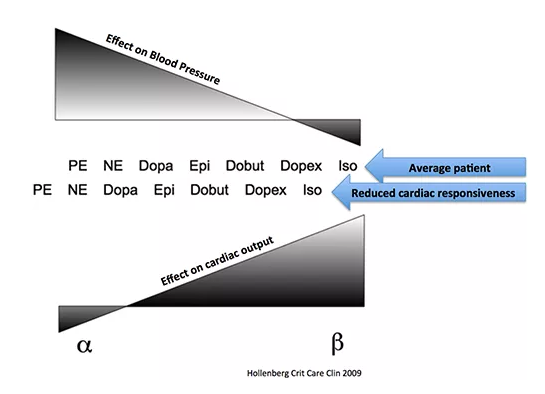
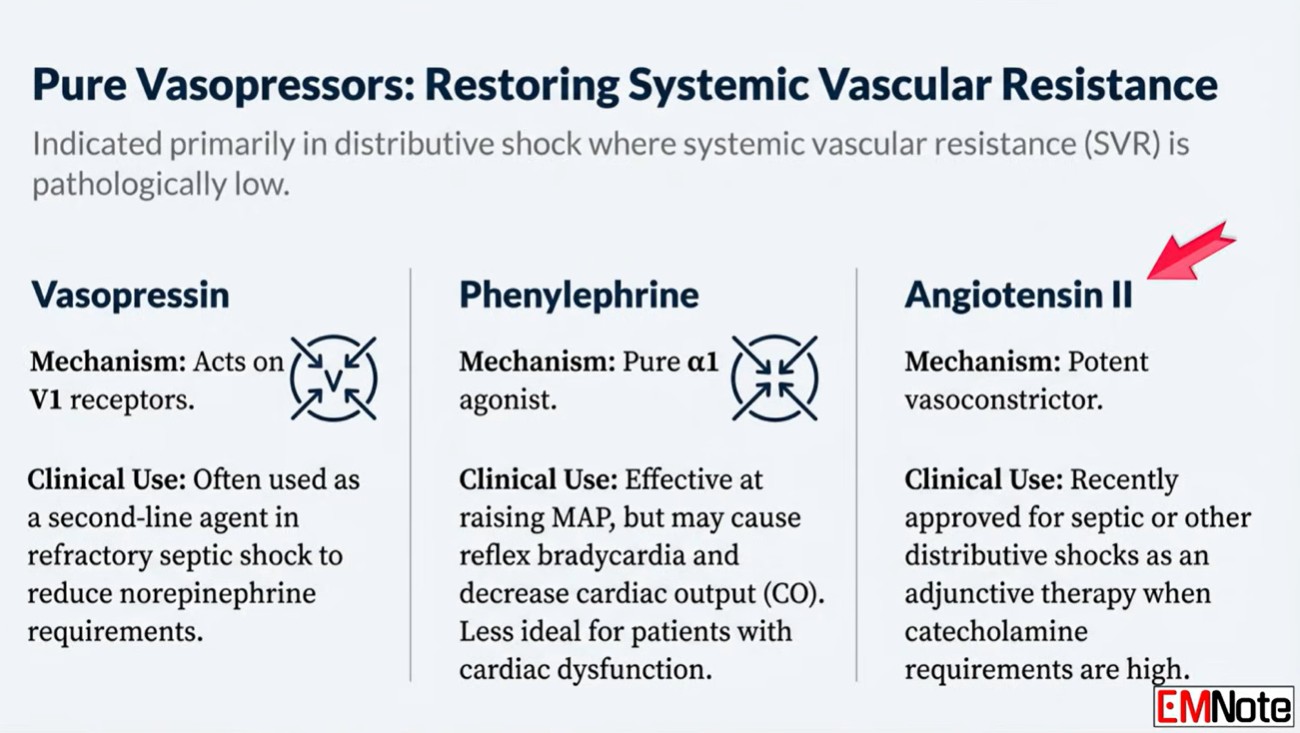
Relative differences in end-organ sensitivity affect the way vasopressors function. For example, norepinephrine typically has predominantly vasoconstrictive effects with a small amount of isotropy. In a patient with reduced cardiac responsiveness to beta-agonist stimulation, this could cause the vasoconstrictive effects of norepinephrine to predominate even further. In this scenario, norepinephrine would have nearly the same effect as a pure vasoconstrictor such as phenylephrine:
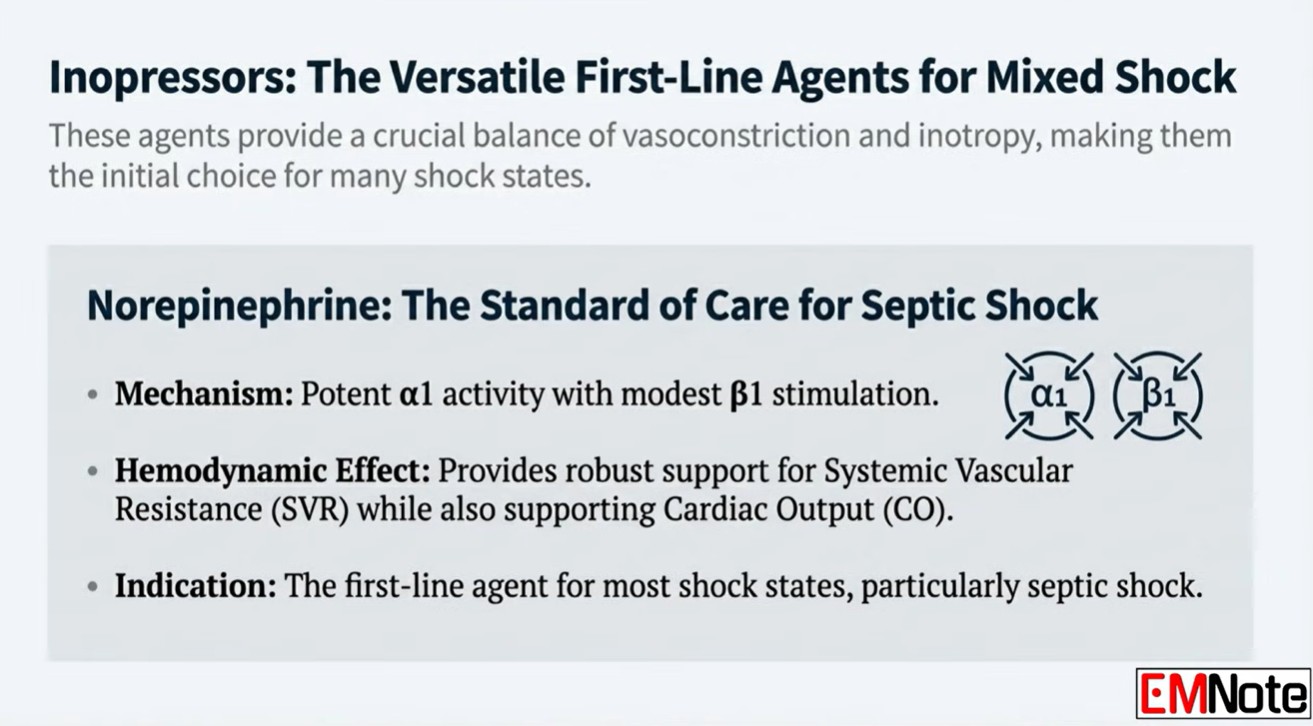
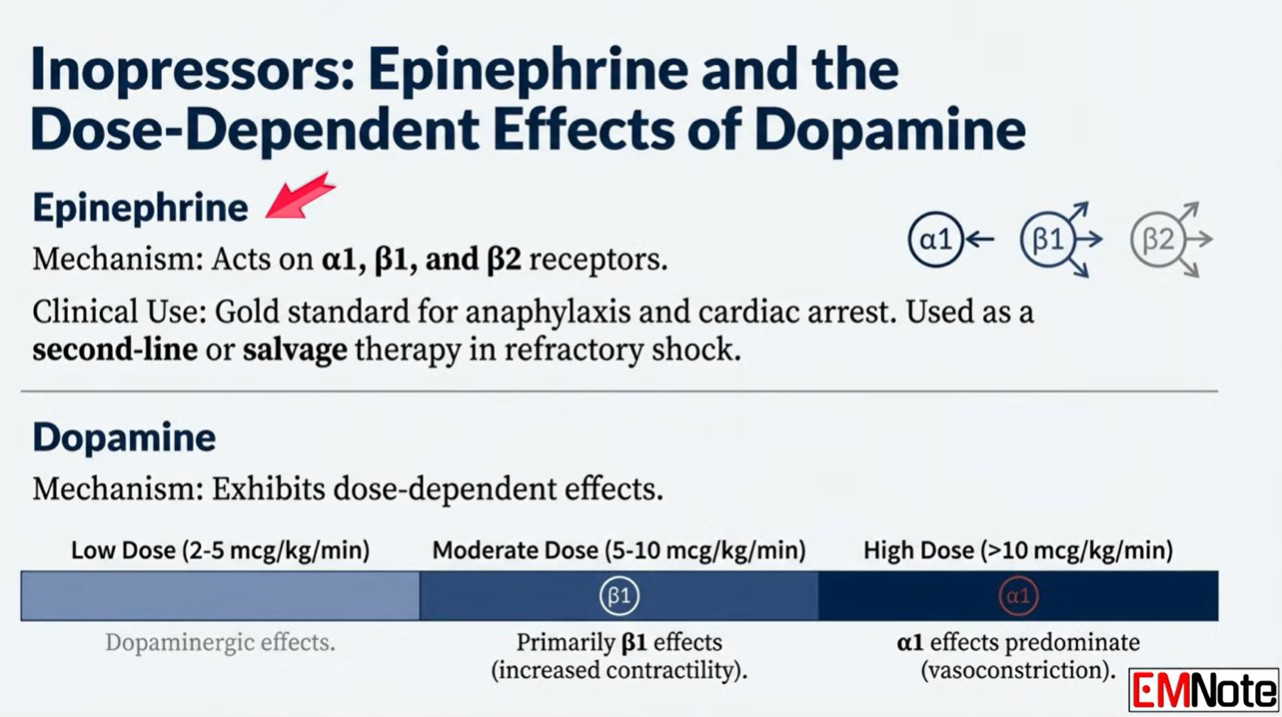
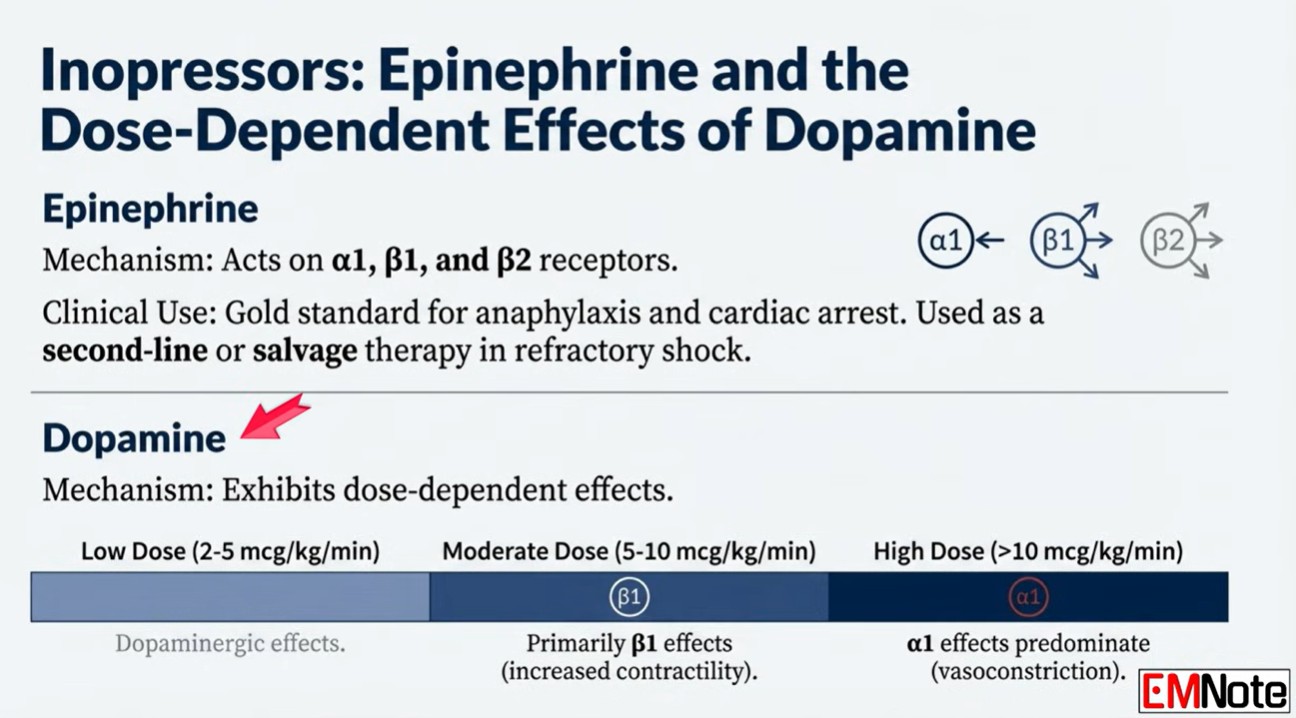
Foundational concept #2: Norepinephrine and epinephrine are both evidence-based vasopressors for use in sepsis.
Although norepinephrine is typically first-line in septic shock, epinephrine is also a reasonable choice.
Groups of patients respond similarly to norepinephrine vs. epinephrine, but this doesn’t mean that individual patients will have the same response to either drug (an assumption exemplifying the flaw of averages). On the contrary, it is likely that some patients respond better to norepinephrine, while other patients respond better to epinephrine.
Groups of patients respond similarly to norepinephrine vs. epinephrine, but this doesn’t mean that individual patients will have the same response to either drug (an assumption exemplifying the flaw of averages). On the contrary, it is likely that some patients respond better to norepinephrine, while other patients respond better to epinephrine.
Foundational concept #3: The epinephrine hyper-responsive patient
Average responsiveness to norepinephrine vs. epinephrine
On average, equal doses of norepinephrine or epinephrine are required to achieve blood pressure targets.
The phenomenon of epinephrine hyper-responsiveness
Some patients seem to be especially responsive to epinephrine, with the following features: (3)
- They don’t respond very well to norepinephrine, often requiring high doses of norepinephrine. Sometimes the norepinephrine dose will fluctuate widely, suggesting that the norepinephrine isn’t very effective. While on norepinephrine, they may have poor perfusion.
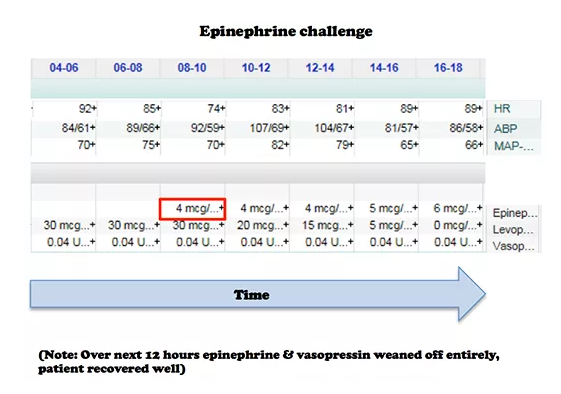
- They are very responsive to epinephrine. For example, the image below shows a patient who was transitioned from 30 mcg/min of norepinephrine to 6 mcg/min of epinephrine. Following transition to epinephrine, these patients often have improved perfusion.
- There is often an increase in lactate levels following the initiation of epinephrine, which is a positive prognostic sign (discussed below)(4).
Why are some patients epinephrine hyper-responsive?
The physiology of epinephrine hyper-responsiveness is likely multifactorial, perhaps with varying contributions from the following factors.
Factor #1: High endogenous alpha-adrenergic tone? A patient who is already quite vasoconstricted may respond poorly to additional exogenous alpha-adrenergic stimulation.
Factor #2: Relative bradycardia? Occasional patients in septic shock are encountered who have inappropriately normal heart rates (e.g. 50-70 b/m), even despite being on norepinephrine. This could relate to a deficiency of endogenous beta-adrenergic tone, or perhaps an over-reactive carotid baroreceptor response to alpha-adrenergic stimulation (5). Regardless, such patients might benefit from the stronger chronotropic effects of epinephrine.
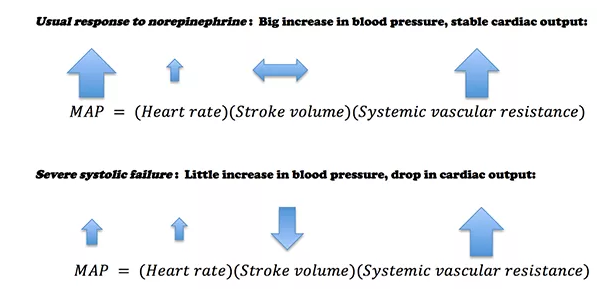
Factor #3: Occult systolic failure? An occasional septic patient has a normal ejection fraction, but after starting norepinephrine the ejection fraction drops. Why? Such patients have likely had systolic dysfunction all along. Initially their untreated vasodilation reduced their afterload, increasing their ejection fraction. Norepinephrine normalizes the afterload, thereby unmasking this systolic dysfunction.
Patients with occult systolic failure may experience less improvement in blood pressure in response to norepinephrine. In extreme cases, their cardiac output could even drop as the norepinephrine is titrated up (6):
Observational studies show that when patients with septic shock are treated with norepinephrine, some experience a decreased cardiac output (Hamzaoui 2010, Meadows 1988, Martin 1999).
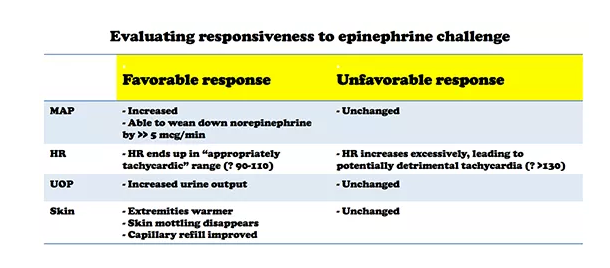
Evaluating epinephrine responsiveness: The epinephrine challenge
Baseline hemodynamics and echocardiography provide static hemodynamic variables which usually cannot predict epinephrine responsiveness (7). Thus, the only way to be certain of how a patient will respond to epinephrine is to administer epinephrine. One potential exception might be a patient with marked tachycardia and a hyperkinetic ventricle.
The best way to determine epinephrine responsiveness may be to simply start a low dose epinephrine infusion (e.g. 4 mcg/min)(8). The patient’s response to epinephrine may be judged based on clinical variables (table below). Although measuring cardiac output could also be performed, this is not my usual clinical practice (9).
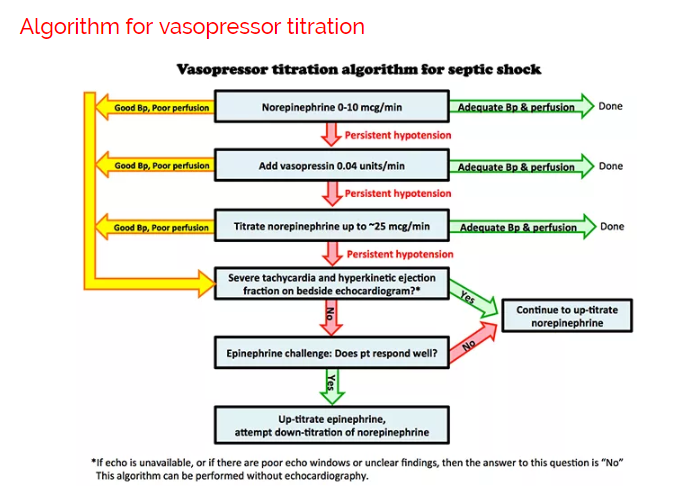
Above is one possible approach to titrating vasopressors in septic shock. Vasopressin is started earlier than in most algorithms (10). More notable features of the algorithm are:
- Epinephrine is trialed relatively early (before the patient is frankly “failing” norepinephrine).
- Many algorithms involve sequential addition of different vasopressors. However, it may also be useful to down-titrate vasopressors to which the patient responds poorly.
Here is an extract of (2) PulmCrit- High dose vasopressors: Never surrender
June 4, 2018 by Josh Farkas but you must read the whole post.And finally after completely reviewing Resource (2)
This post is for use by only the most expert of clinicians – in a critical access hospital I would only consider using this strategy with help and agreement from the critical care specialist at the tertiary care where the patient is being transferred to.
Caution about using high-dose vasopressors
The above studies [reviewed in Dr. Farkas post] show a strong correlation between high-dose vasopressors and mortality. This is probably because the need for high-dose vasopressors correlates with greater disease severity, not because high-dose vasopressors cause mortality. Nonetheless, the need for high-dose vasopressors should never be taken lightly. This is generally a treatment of last resort. Whenever high-dose vasopressors are needed, meticulous evaluation is needed (ideally including echocardiography) with particular attention to the following questions:
- Is blood pressure truly that low? Consider placement of a femoral or axillary arterial catheter to transduce central arterial pressure.
- Is there a role for volume resuscitation or inotropic support? Some patients who respond poorly to norepinephrine may do better with epinephrine (see: epinephrine challenge).
- Is there occult right ventricular failure that could be treated (e.g. with pulmonary vasodilation)?
- Is there low cardiac output and impaired perfusion (e.g. mottling)? In that case, additional vasoconstriction may simply aggravate matters.
- Is there a failure of surgical source control or incorrect antibiotic selection?
- Is the patient on adequate adjunctive therapy (stress-dose steroid, possibly thiamine/ascorbate)?
- Is there a pH abnormality that merits correction (e.g. treatment of hyperchloremic metabolic acidosis with bicarbonate)?
- Is there autoPEEP or elevated intra-abdominal pressure which is impairing venous return?
- Is the patient on any medications which may be reducing the blood pressure (e.g. propofol, dexmedetomidine)?
- Is there clinically significant hypocalcemia?
Having reviewed Resources (1) and (2) above it is a good idea to listen to Dr. Weingart’s podcast Resource (3) Podcast 87 – Mind of the Resuscitationist: Stop Points [things to consider when you need to add a second vasopressor] November 26, 2012. This podcast reinforces with a clinical case, the points that Dr. Farkas made above in his posts.
Here are some excerpts from Dr. Weingart’s Stop Points podcast:
When you’re getting ready to add a second vasopressor, these are the points to consider and things to do:
Stop Points
- Volume – [Are you sure the patient is adequately volume loaded]
- Calcium – [Check the ionized calcium as catecholamines won’t work in the face of low ionized calcium]
- Bleeding – [Is there occult bleeding that you haven’t diagnosed yet]
- Adrenal Insufficiency – [Consider stress dose of IV Solu-Cortef]
- Hypothyroidism – [See Myxedema Coma or Crisis
Updated: Mar 27, 2017 and Myxedema Coma or Crisis Treatment & Management Updated: Mar 27, 2017 from emedicine.medscaape.com.- Wacky stuff [Listen to the podcast]
Next Dr. Weingart states you should perform a RUSH exam [Link is to his show notes and podcast – definitely want to review this.
Resources:
(1) PulmCrit- Epinephrine challenge in sepsis: An empiric approach to catecholamines April 25, 2016 by Dr. Josh Farkas
(2) PulmCrit- High dose vasopressors: Never surrender
June 4, 2018 by Josh Farkas(3) Podcast 87 – Mind of the Resuscitationist: Stop Points
November 26, 2012 by Scott Weingart(4) EMCrit 201 – Deeper on Vasopressors and Athos 3 with Mink Chawla
June 12, 2017 by Scott WeingartLinks To EM Quick Hits 18 Conservative Management Pneumothorax, Microdosing Buprenorphine, Practical Use of CRITOE, Canadian TIA Score, Pediatric Surviving Sepsis Guidelines, Safety of Peripheral Vasopressors Posted on September 29, 2021 by Tom Wade MD
Topics in this EM Quick Hits podcast
Justin Morgenstern on watchful waiting for large spontaneous pneumothoraces (0:44)
Michelle Klaiman on mirco-dosing buprenorphine for opiate use disorder (5:17)
Arun Sayal on the practical application of CRITOE in pediatric elbow fractures (10:45)
Jeff Perry on The Canadian TIA Score (19:37)
Sarah Reid on updated pediatric surviving sepsis guidelines (25:59)
Salim Rezaie (Best of REBELEM) on safety of vasopressor administration through peripheral IVs (33:40)
Link To “EM Quick Hits 7 Approach to Status Epilepticus, Codeine Interactions, Anticoagulation in Malignancy, Atrial Fibrillation Rate vs Rhythm Control, Peripheral Vasopressors, Motivational Interviewing”
Posted on January 16, 2020 by Tom Wade MDAnd here is the timeline for the podcast:
Topics in this EM Quick Hits podcast
Anand Swaminathan on a simple approach to status epilepticus (0:31)
David Juurlink on codeine and tramadol interactions: nasty drugs with nastier drug interactions (8:37)
Brit Long on DOACS in patients with malignancy: which patient’s with cancer can be safely prescribed DOACs? (13:05)
Ian Stiell on atrial fibrillation rate vs rhythm control controversy (20:55)
Justin Morgenstern on peripheral vasopressors: safe or unsafe? (26:39)
Michelle Klaiman on motivational interviewing that makes a difference to patient’s lives (33:56)
Linking To And Embedding EM Note’s “Vasopressors and Inotropes for Shock Management”
Posted on April 25, 2026 by Tom Wade MDNote: In addition to today’s resource, every clinician responsible for emergency care should purchase and carefully review PressorDex®: Critical Care Medications Guide, 5th Edition, 2024. It is an outstanding resource to always have immediately available.
EM Note is an outstanding podcast series. You can access the complete list (currently 683) at EM Note Podcast.
Today, I review, link to, and embed EM Note‘s Vasopressors and Inotropes for Shock Management.
All that follows is from the above resource.
0:06
Vasopressors and Inotropes for Shock Management
0:14
0:44
1:15
1:25
1:37
1:58
2:22
2:46
3:13
3:47
3:59
4:17
4:56
5:25
5:42
6:32
7:03
7:44
8:13
9:07
9:24
9:50
Vasopressors and Inotropes for Shock Management
Dec 29, 2025 EMNote PodcastEM Note Newsletter https://forms.gle/8boToiKDXVE3V8U19 Signup to get free weekly PDF via email. PS: Please join our membership for more perks (members can request for specific PDF file by posting in the EM Note YouTube Membership section).
Membership: https://tinyurl.com/joinemnote
This entry was posted in EM Note, Vasopressors, Vasopressors and Inotropes for Shock Management. Bookmark the permalink.Linking To And Excerpting From “The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults” From RebelEM
Posted on February 13, 2025 by Tom Wade MDToday I review and excerpt from “The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults“* from RebelEM. June 8, 2023. Written by Courney Knieriem, MD
REBEL Crit, REBEL EM
Medical Category: Cardiovascular, Resuscitation*Courney Knieriem, MD, “The Safety and Efficacy of Push Dose Vasopressors in Critically Ill Adults”, REBEL EM blog, June 8, 2023. Available at: https://rebelem.com/the-safety-and-efficacy-of-push-dose-vasopressors-in-critically-ill-adults/.
All that follows is from the above resource.
Background Information:
Acute Hypotension is associated with increased morbidity and mortality. Continuous vasopressor infusions have previously been the mainstay of treatment. However, peripherally dosed push dose pressors, (PDPs), are beginning to be administered more frequently for management of acute hypotension.1-4 The PDPs, phenylephrine and epinephrine, result in vasoconstriction and increased cardiac contractility. They can be associated with side effects such as reflex bradycardia, decreased stroke volume in phenylephrine, tachycardia and hypertension associated with epinephrine. The authors of this trial sought out to describe PDP and assess the efficacy and safety of PDP use in the management of hypotension. Prior literature primarily focused on safety and medication errors, and while this study did the same, they also assessed variables associated with PDP response. Paper: Singer S, et al. The safety and efficacy of push dose vasopressors in critically ill adults. Am J Emerg Med. 2022 Sep 5. PMID: 36108346
Clinical Question:
What is the efficacy and safety of peripherally administered push dose pressors for the treatment of acute hypotension?
What They Did:
- Single-center, retrospective cohort study performed at a single academic medical center
- Cohorts were analyzed according to PDP response (responders vs non-responders)
- Analyzed PDP administration in the setting of acute hypotension. Assessed clinical practice, outcome, length of stay, safety, and efficacy of both phenylephrine and epinephrine peripherally administered through a push dose.
- Epinephrine – 10ug/mL, 10mL syringe*
- Phenylephrine – 100ug/mL, 10mL syringe*
- Phenylephrine bolus doses from 100-200ug and epinephrine 10-20ug administered every 2-5 minutes pursuant to provider order
*The study used premixed syringes which the authors strongly recommend.
Inclusion Criteria:
- Adults age >18 years old
- Received at least one bolus dose of phenylephrine or epinephrine pre-filled syringes
Exclusion Criteria:
- Operating room patients
- Patients with any of the following:
- Priapism
- Epistaxis
- Missing vital signs within 1 hour of PDP dose
- Received both Epinephrine (Epi), and Phenylephrine (PE) were excluded
Outcomes:
Primary
- Efficacy, defined as a systolic BP increase of 25% post PDP administration
- Responder – Episodes that achieved a > 25% increase in SBP were classified as responders
- Nonresponder – Episodes that achieved a < 25% increase in SBP were classified as responders
Safety
- HTN (BP>180/110) within 1 hour PDP
- Bradycardia within 1 hour of Phenylephrine
- Tachycardia (>30% increase in HR from baseline within 1 hr of epi)
Additional Outcomes
- Delta of SBP/DBP 1 hour pre/post
- Requirement of a dose increase of continuous vasopressor support within 4 hours of PDP administration
- Cardiac arrest within 1 hour of PDP
- ICU/Hospital length of stay
- In hospital mortality
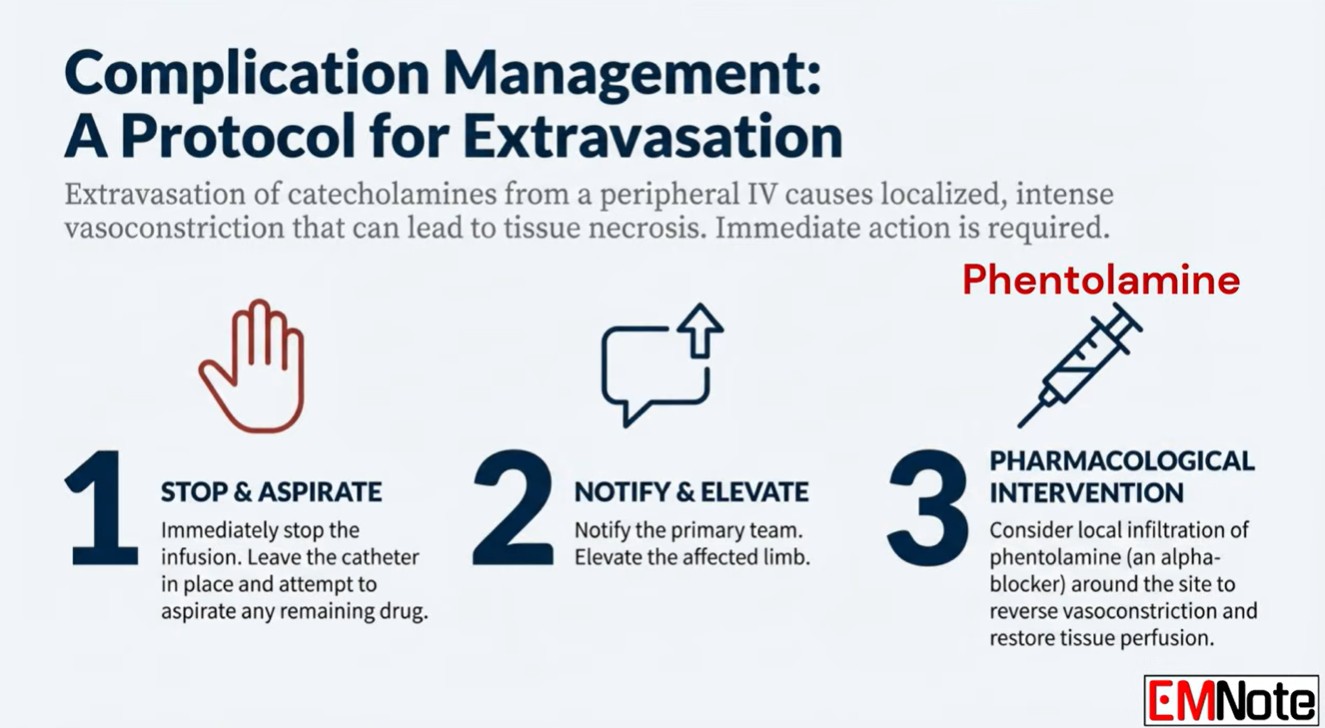
- Extravasation
- Severe adverse events such as:
- Administration of atropine for bradycardia within 1 hr of phenylephrine
- Hypertension requiring an anti-hypertensive within 1 hr of epinephrine
Results:
- 1727 patients (n=2183 PDP episodes) were included in the final analysis.
- 3175 patients evaluated for inclusion however 1348 excluded due to PDP being given in OR as the main reason for exclusion
- Median dose of phenylephrine = 400mcg (Range 200 to 888mcg) and Epinephrine = 50mcg (Range 20 to 100mcg)
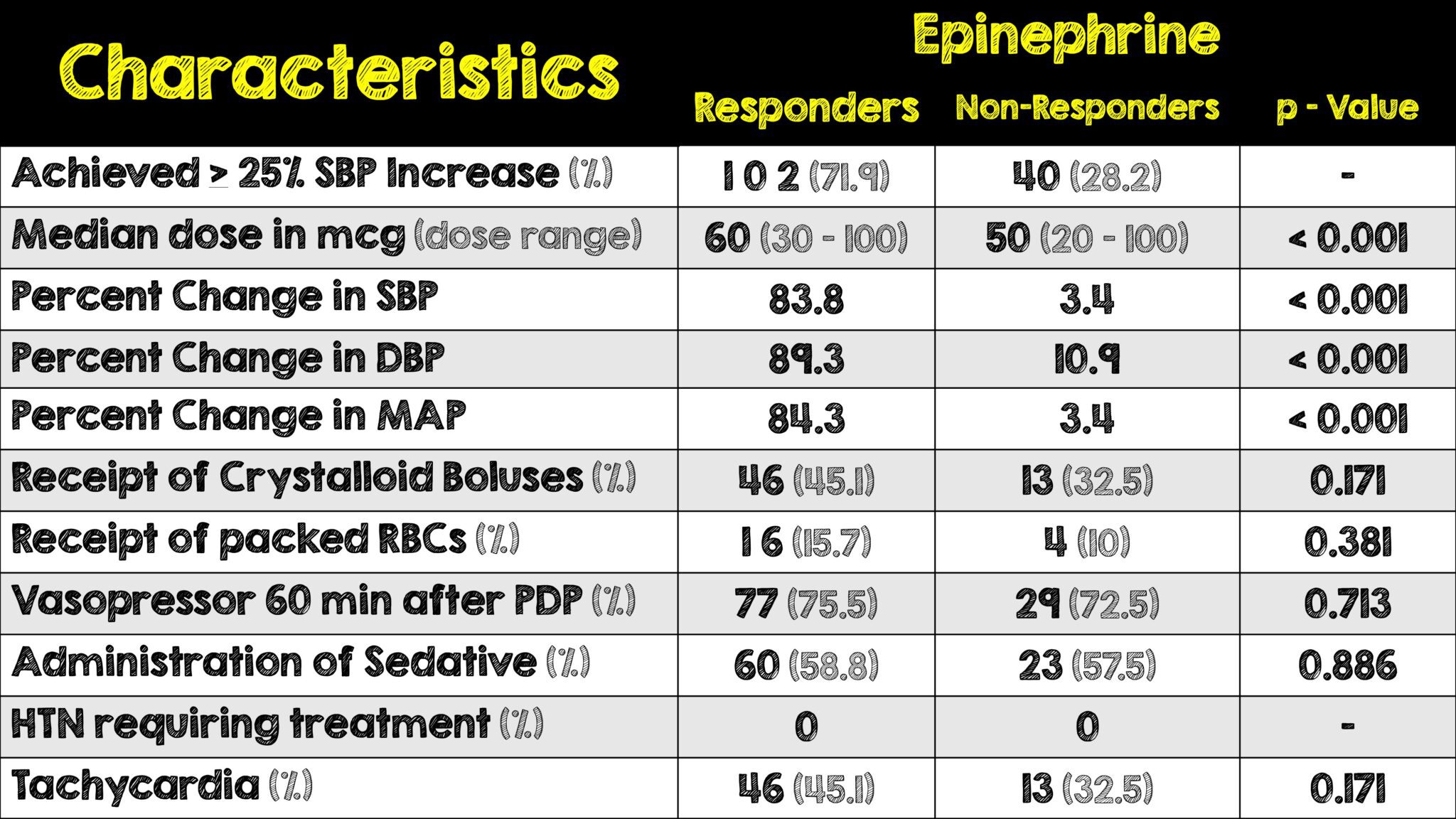
- Primary outcome achieved in 71.8% (102) pts in the epi group and 55.9% (1140) pts in the phenylephrine group
Critical Results:
- The odds ratios in the chart above apply to phenylepinephrine responders, the following values apply to non-responders
- Receipt of crystalloid boluses: OR 0.0639; 95% CI 0.432 to 0.946
- Receipt of PRBCs: OR 0.303; 95% CI 0.099 to 0.935
- Phenylepinephrine responders more frequently received pRBC, crystalloid boluses and sedation
- No serious adverse events occurred in the epinephrine cohort
- History of CHF associated with response to epinephrine (OR 11.889, 95% CI 1.030 – 137.257)
- Neither cohort had any adverse extravasation requiring phentolamine or terbutaline
Discussion:
- There is a recent “push” to utilize “Push dose pressors” as the correction of acute hypotension in a variety of clinical scenarios. This study chose a relevant topic to analyze that could influence acute management in the ED and has a fairly larger sample size of patients to do so.
- Phenylephrine and epinephrine are two of the most common vasopressors and more studies need to be done to analyze long term effects of the two.
- The retrospective design of this study omitted assessment of ventricular dysrhythmias related to push dose pressor administration, as they were reliant on information in the EMR. Adrenergic agonists certainly have the potential to affect sympathetic sequelae, and adverse events. Further studies are needed to assess the prevalence of cardiac dysrhythmia.
- Overall, 56% of patients that received phenylephrine and 70% of patients that received epinephrine achieved a 25% increase in SBP. Both agents improved SBP, DBP, and MAP. The increase in metrics was expected, however, it is worth noting that epinephrine seems more effective……..
- Not so fast…15.5% in phenylephrine group and 27.5% in the epi group received continuous vasopressor infusions within 50 min prior to PDP and 46.3% in the phenylephrine group and 74.6% in the epi group received continuous vasopressor infusions within the 60min after PDP administration….both would favor epi seeming more effective
- Administration of crystalloid boluses and PRBCs were associated with a lack of response to phenylephrine. This could indicate that hypotension may have been adequately managed with preload expansion. Another study showed similar results, >30mL/kg of fluids prior to phenylephrine administration received fewer and lower cumulative phenylephrine dose.5, 6 These findings highlight the importance of adequate preload expansion in the treatment of acute hypotension.
- Administration of any sedative was predictive of phenylephrine response. This could be useful in RSI, where sedatives are frequently used before intubation. The mechanism of peri intubation hypotension is multifactorial including vasoplegia, loss of adrenergic tone, worsening acidosis due to apnea, and reduced venous return after initiation of positive pressure ventilation
- Epinephrine concentrations diluted at bedside showed less hemodynamic events. This highlights the importance of pre-made PDP syringes andproper labeling, storage, and staff education for PDPs.
- The low adverse event rate that occurred in this study should emphasize the importance of premade PDP syringes, proper labeling, storage, and staff education when using PDPs
- Caution should be taken when utilizing PDPs in patients with cardiac dysfunction or congestive heart failure. Lastly, bedside dilutions of epinephrine had less efficacy thus highlighting the importance of pre-made syringes, proper labeling, storage, and staff education regarding PDPs.
- In regards to the role of PDP in patients with cardiac dysfunction and CHF, this study found no differences in response to either agent in patients with cardiac dysfunction. Interestingly, CHF history was associated with a positive response to epinephrine. Unfortunately, due to the small sample size of the epinephrine cohort, further studies are warranted to determine the effects of cardiac dysfunction on PDP response.
- Caution should be taken when utilizing PDPs in patients with cardiac dysfunction or congestive heart failure. Lastly, bedside dilutions of epinephrine had less efficacy thus highlighting the importance of pre-made syringes, proper labeling, storage, and staff education regarding PDPs.
Author’s Conclusions:
This study demonstrates that PDP phenylephrine and epinephrine are safe and efficacious in treating the acute hypotensive period
Our Conclusion:
Although conclusions on mortality and clinical outcomes cannot be definitively made, this retrospective study demonstrates the safe and efficacious use of PDP in the acute hypotension period with no severe adverse effects.
Potential to Impact Current Practice:
Initiatives should be made at the institution level to develop in-service education sessions, policies and procedures for the safe administration of PDPs in the acute hypotensive period. If pre-made syringes are not financially feasible then the creation of these medications should be done by a dedicated emergency department pharmacist.
References:
- Singer S, et al. The safety and efficacy of push dose vasopressors in critically ill adults. Am J Emerg Med. 2022 2022 Sep 5. PMID: 36108346
- Cole JB, et al. Human Errors and Adverse Hemodynamic Events Related to “Push Dose Pressors” in the Emergency Department. J Med Toxicol. Epub 2019 Jul 3. PMID: 31270748
- Maheshwari K, et al. The relationship between ICU hypotension and in-hospital mortality and morbidity in septic patients. Intensive Care Med. 2018;44(6):857–67. PMID: 29872882
- Jones AE, et al. Emergency department hypotension predicts sudden unexpected in-hospital mortality: a prospective cohort study. Chest. 2006;130(4):941–6. PMID: 17035422
- Holler JG, et al. Nontraumatic hypotension and shock in the emergency department and the prehospital setting, prevalence, etiology, and mortality: a systematic review. PLoS One. 2015;10(3):e0119331. PMID: 25789927
- Schwartz MB, et al. The impact of push-dose phenylephrine use on subsequent preload expansion in the ED setting. Am J Emerg Med. 2016; PMID: 27720568
For More Thoughts on This Topic Checkout:
- EMCrit: Push-Dose Pressures Update
- EMDOCS: Push-Dose Pressures – An Update for 2019
- Alabama Chapter of the American College of Emergency Physicians (alacep.org)
Post Peer Reviewed By: Salim R. Rezaie, MD (Twitter: @srrezaie)
This entry was posted in Peripheral Push Dose Pressors, Pharmacy Practice, Push Dose Pressors, REBELEM. Bookmark the permalink.“Pulse Dose Pressors For Children And Adults From Dr. Mellick’s Blog
Posted on December 1, 2023 by Tom Wade MD