
[Update 9-5-2018 be sure read and watch EMCrit 231 – How to Practice Cricothyroidotomy (Cric) August 25, 2018 by Dr. Weingart. It is awesome.]
As with most things about Advanced Life Support that I have reviewed in the last six months, since I discovered EmCrit [which has actually been on the internet for five years], these resources are all from Dr. Scott Weingart’s outstanding podcast series EmCrit.
This post is really just to remind me of the location of these resources on the internet and to help fix his teaching in my mind.
The best thing to do is to go directly to Dr Weingart’s All Things Cricothyrotomy Podcast 131 show notes. There are an incredible list of resources including Dr. Weingart’s outstanding thirty minute video that he gave at SMACC 2014. And after reviewing Podcast 131 go on to review Podcast 119 which is contains the video from Dr. Rich Levitan.
I have made some notes below on Dr. Weingart”s and on Dr. Levitan’s talks (after the videos) to help fix them in my mind and for quick review.
I’ve included three of the videos from Podcast 131 just so I can easily review them:
First is Dr. Weingart’s thirty minute lecture on the 10 Ways We Fail At Cricothyrotomy.
Here are the notes I made from the above talk:
Notes from Dr. Weingart’s Podcast 131
10 Ways Not to Mess This [Cricothyrotomy] Up
1. Be Mentally Prepared To Make the Cut
For every airway: Realize that every airway is a potential surgical airway.
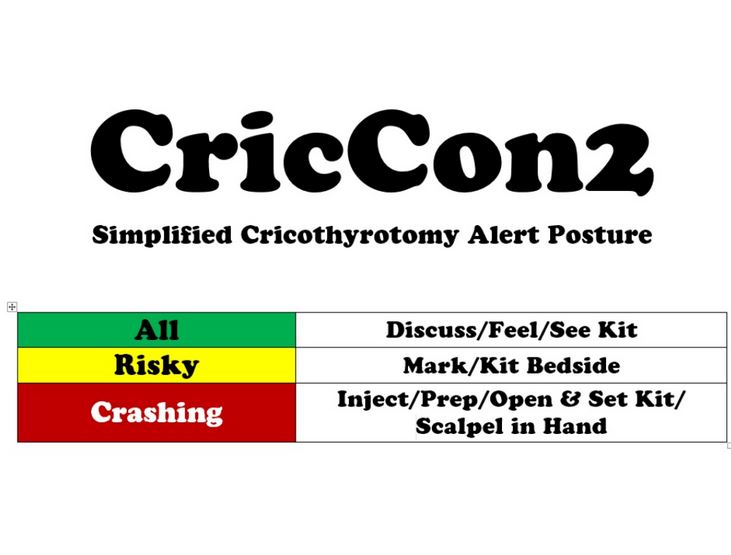
All-So for every airway Discuss Your Plan (ABCD)/Feel the neck/And See the Cric kit.
Risky-If you think the airway is risky, mark the neck and have the cric kit by the bedside.
You do it with a black sharpie marker. This lets everyone know that this is the next step and that if you do it (the cric) it is not because you screwed.
Crashing-Open and Set up the Kit and have scalpel in hand at the ready as someone else is
managing the airway from above.
2. You Have to be the backup.
3. You need to know the anatomy.
STAY IN THE MIDLINE–As long as you do, there won’t be any vascular catastrophies.
We err by going too high. If you are going to err, err by going too low.
“If you can’t find what you want stay right by the sternal notch, go a couple of centimeters
up and try cutting there.
We feel (palpate) wrong. Sometimes we just can’t feel anything. If you start low, the first
structure you will feel popping out is the cricoid membrane. And right above that is the
thyroid cartilege.
But if you can’t find anything, find the sternal notch and that will tell you where midline is
and where to cut.
Don’t start at the top and work your way down.
Start at the bottom and work your way up.
4. We are afraid of blood.
This is a bloody procedure. This is a procedure that is not visual; it is tactile.
Once you make that first cut through skin, there will be bleeding.
You cannot rely on your eyes at that point.
You can’t waste time suctioning that blood attempting to get a view.
Don’t be scared of bleeding. As long as you don’t cut the carotid, any bleeding there is
totally controllable.
The way to stop the bleeding is to finish the procedure.
Get the tube in and then any bleeding you caused is totally responsive to direct pressure.
Do not stop for the bleeding. That is a mistake.Don’t have your friends shoving in a bunch of 4 by 4s.
There is nothing dangerously vascular in the midline.
Although it looks awful, the patient cannot exsanguinate from this incision.
5. We injure ourselves or are team by exposure to blood.
There will be blood sprayed everywhere.
Therefore you and every member of the team must be wearing a mask and eye protection.
You and everyone on the team must take the time to do this before you cut.
Do not cut yourself or any member of your team!
6. We regress to a misperception of safety and familiarity.
Don’t use the needle and the wire–it just won’t work. Use the scalpel.
7. We can fail by using the wrong surgical technique, the standard surgical technique. It works but there are so many points of failure.
In the old days, there was a huge failure rate for cricothyrotomy. And most of those failures were because at some point we had to take our instrument out of the cricothyroid membrane and then blindly stick a tube in. And those tubes went into all sorts of weird places and the patient’s neck would blow up like the Michelin man. This does not work; this is not acceptable anymore.
Instead, I recommend bougie guided cricothyrotomy. This emerged from the battlefield where they have to get it right even when stressed.
Bougie guided cric is what I teach and it is the only technique I use now.
And I use a variant called the scalpel-finger-bogie method.
You take your scalpel and you make two cuts.
You make a cut from the thyroid prominence to the bottom of the cricoid. And that is if you can feel the anatomy.
If you can’t feel the anatomy, go all the way from the sternal notch to two-thirds up on the
neck. Make a great big incision. The worse the situation, the bigger the incision can be.
And now you are going to make a second cut; it is actually two cuts.
You are going to plunge that scalpel through the cricothyroid membrane and you are going to pull [the scalpel] towards you. Turn the scalpel blade around and push away from you.
And what if you plunge too far? You can’t. If you are through the cricothyroid membrane there is cartilege in back that will prevent you from going too far. If you are in the right place, you can’t cut laterally too far, you can’t cut posteriorly too far.
[This isn’t true if you are below the cricothyroid membrane, there is no cartilege
and you can go to far in and you could go too far latterally. Same is true if you go too high
and mistakenly go through the thyro-hyoid ligament.]
You can’t mess it up if you are in the right place.
So you plunge the knife in and pull it toward you and then push it away from you.
And now you are going to put your finger in.
The finger serves a bunch of purposes.
When you plunge in, don’t do it a little bit so that you just feel the cartilege on both
sides.
Plunge as far as your finger will go.
And what your finger will touch is the posterior wall of the cricoid cartilege.
And now you will know without a shadow of a doubt that you are in the right place because you have cartilege all circumferentially around your finger and then the tip of your finger
touches that posterior cricoid.
You can not be anywhere else in the airway. No matter how much blood there is, you know that you are where you need to be.
And now you have dilated that incision to the exact size you need to put in a small
endotracheal tube or a trach through that hole.
You are now set at this point and your pulse rate should dramatically drop because everything is going to be okay.
But then we add in the boogie.
We ride the boogie along our finger. We feel the boogie go exactly where our finger is and we feel it pass our finger to go down into the airway.
And now the boogie will be the conduit that forces the endotracheal tube to go into the right place. It can’t go anywhere else.
You can corkscrew the 6.5 ET [Dr. Brainnard recommends 6.0] tube down the boogie. And you can push as hard as you want because it is going to be forced to go where it needs to go.
At 18:51 to 21:13 Dr. Weingart shows his video of the scalpel-finger-boogie.
And then from 21:20 to 21:50 Dr. Weingart shows the second video of his talk..
Misplaced tube:
The other way we fail is misplaced tube. The boogie is solution to that. Or Dr Levitan will
show you his cric key. That is the solution to that. You can’t be blindly putting these tubes.
If you feel that boogie go past the sternal notch and get hold up, that is secondary
confirmation that tells you you are in the right place. It can’t be anywhere else.
You can’t somehow of gotten it in the esophagus, if the boogie went past the sternal notch and got hold up. The boogie stops.
8. Can’t feel any antomy
Sometimes you can’t feel any surface anatomy. And if that stops you that is a huge problem.
It shouldn’t. In that case, you are going to spread all of the soft tissue. And then cut to air.
What does that mean?
It means that you are making a huge skin incision. It could be all the way up the neck, I
don’t care.
And then you get two fingers in on either side, or you have an assistant do it, and you start
spreading the tissue out of your way.
And you keep sticking your finger in until you feel cartilege-trachea anatomy.
And then you will continue the procedure.
At 23:20 to 23:55, Dr Weingart shows another brief video
from Andrew Hirsch (sp?)
Dr. Hirsch says:
“You are going to make a midline incision up to 8 to 10 cm to the depth of the strap muscles.
The anesthetist should then insert the fingers of both hands and bluntly dissect and seperate these muscles.these muscles, keeping in mind that the trachea may not be in the midline.
Airway structures should then be identified and stabalized.”
Dr. Weingart says while the video is running:
“Just spread, spread, spread. Keep spreading. Keep spreading. And stick your finger in.
Eventually you will find criccoid–thyroid–trachea.”
“You will find things that feel cartilagenous.”
“There is nothing else in the neck that is cartilagenous.”
“There is nothing else in the neck that has rings.”
“You cannot destroy things with your fingers. They are the safest tool in operative
procedure.”
“Just keep on spreading. You will find it, I promise.”
“You will not rip asunder the carotid and the IJ. You will be okay. Keep spreading until you
feel something with your finger.”
9. We fail to train.
You have to train on this procedure.
But you can do a hundred of these in training with very little equipment.
You can make a simple cric trainer. Here is the picture below:
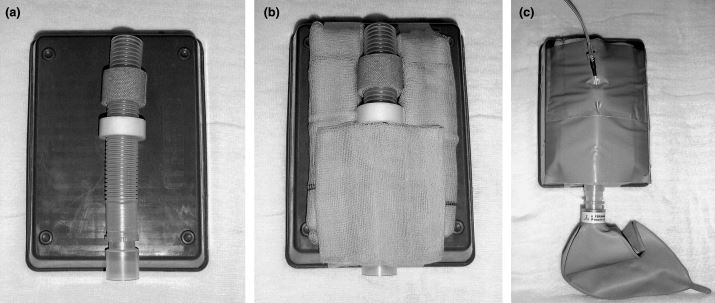
This isn’t perfect. But it gives you the skills, it gives you you the mindset you need.
This simple inexpensive do-it-yourself version works.
And if you take this and put it in the mental simulator it will really help
“This will get you very close to where you need to be,” Dr. Weingart states.
10.We fail to consider the awake cricothyrotomy.
Next are links to Dr. Weingart’s next two videos [I couldn’t embed them but they need to be watched!]
Scalpel Finger Bougie Cricothyrotomy for SMACC 2014 [Direct link to video on Vimeo]
Emergency Surgical Airway [Direct link to video on Vimeo]
Next I will review again Podcast 119.
Podcast 119 – Rich Levitan on the Surgical Airway
March 10, 2014 by emcrit [Show notes which contain Dr. Levitan’s Videocast]
This is an outstanding videocast and can profitably be watched over and over; However, the scalpel-finger-bougie method which Dr. Weingart demonstrates in his three videos above is safer (less danger of creation of a false passage which can occur even with bougie) than what is demonstrated in Dr. Levitan’s video.
22:35 to 23:10 We watch how EM and ENT specialist Dr. William Levin performs a cadaver cricothyrotomy.
23:10 to 24:10 We watch Dr. Levitan perform a cadaver cricothyrotomy.
26:22 Dr. Levitan’s take home points: 1. Surgically inevitable airway [Go ahead and do it!], 3. Cartalginous Cage [Understand how this anatomy helps you make your incision through the cricoithyroid membrane safely], 4. Sternal Stabalization [Stabilize your dominant hand, the knife hand (the cutting hand) on the sternum].
20:00: Realize that pneumothorax is what can kill your pt after surgical airway. So think of this if pt crumps. [And reach for the ultrasound scanner or for the scalpel for open thoracostomy if the situation is extremely urgent].
The distance from vocal cords to the carina averages 11 cm. At the cricothyroid membrane you are below the cords hence the distance to the carina is even less.
Use a 6.0 mm ID endotracheal tube for use through the cricothyroid membrane. Dr. Levitan recommends using a #20 blade to generate a big opening.
The pilot tube comes off at 14 cm and so it is easy to pass the tube too far and end up ventilating only one lung.
EMCrit Podcast 131 – Cut to Air: Surgical Airway from SMACC Gold
August 26, 2014 by emcrit [Show notes which contain links to Eleven Outstanding Videos on Cricothyrotomy. All need to be watched and carefully thought about before you claim your CME credit (if you want to get the maximum learning value.)]
Bougie-Aided Cricothyrotomy by Darren Braude
April 13, 2010 by emcrit [Show notes contain link to the video]
How to Build the Ultimate Cricothyrotomy Trainer with Chris Bond
January 31, 2013 by emcrit [Show notes contain link to the video]
Additional Resources:
(1) Emergency surgical cricothyroidotomy: 24 successful cases leading to a simple ‘scalpel-finger-tube’ method. [PubMed Abstract] Emerg Med Australas. 2012 Feb;24(1):23-30.



