In this post, I link to and excerpt from The American College of Radiology’s ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. J Am Coll Radiol. 2017 May;14(5):587-595. doi: 10.1016/j.jacr.2017.01.046. Epub 2017 Apr 2.
The above article has been cited by 490 articles in PubMed Central.
There are 289 similar articles in PubMed Central.
All that follows is from the above resource.
Abstract
Thyroid nodules are a frequent finding on neck sonography. Most nodules are benign; therefore, many nodules are biopsied to identify the small number that are malignant or require surgery for a definitive diagnosis. Since 2009, many professional societies and investigators have proposed ultrasound-based risk stratification systems to identify nodules that warrant biopsy or sonographic follow-up. Because some of these systems were founded on the BI-RADS® classification that is widely used in breast imaging, their authors chose to apply the acronym TI-RADS, for Thyroid Imaging, Reporting and Data System. In 2012, the ACR convened committees to (1) provide recommendations for reporting incidental thyroid nodules, (2) develop a set of standard terms (lexicon) for ultrasound reporting, and (3) propose a TI-RADS on the basis of the lexicon. The committees published the results of the first two efforts in 2015. In this article, the authors present the ACR TI-RADS Committee’s recommendations, which provide guidance regarding management of thyroid nodules on the basis of their ultrasound appearance. The authors also describe the committee’s future directions.
Keywords: Thyroid nodule; management guidelines; thyroid cancer; ultrasound.
Copyright © 2017 American College of Radiology. Published by Elsevier Inc. All rights reserved.
Introduction
Thyroid nodules are exceedingly common, with a reported prevalence of up to 68% in adults on high-resolution ultrasound [1]. Currently, fine-needle aspiration (FNA) is the most effective, practical test to determine whether a nodule is malignant or may require surgery to reach a definitive diagnosis [2]. However, most nodules are benign, and even malignant nodules, particularly ones smaller than 1 cm, frequently exhibit indolent or nonaggressive behavior [3, 4, 5]. Therefore, not all detected nodules require FNA and/or surgery.
Despite a rapid increase in the reported incidence of papillary thyroid cancer that resulted from screening thyroid sonography in asymptomatic patients in South Korea, mortality has remained extremely low [6]. In the United States, overdiagnosis of thyroid cancer, defined as “diagnosis of thyroid tumors that would not, if left alone, result in symptoms or death” accounted for 70% to 80% of thyroid cancer cases in women and 45% of cases in men between 2003 and 2007 [7].
Therefore, a reliable, noninvasive method to identify which nodules warrant FNA on the basis of a reasonable likelihood of biologically significant malignancy would be highly desirable. In 2015, committees convened by the ACR published white papers that presented an approach to incidental thyroid nodules and proposed standard terminology (lexicon) for ultrasound reporting [8, 9]. The purpose of the present white paper is to present our system for risk stratification, which is designed to identify most clinically significant malignancies while reducing the number of biopsies performed on benign nodules.Overview of ACR TI-RADS
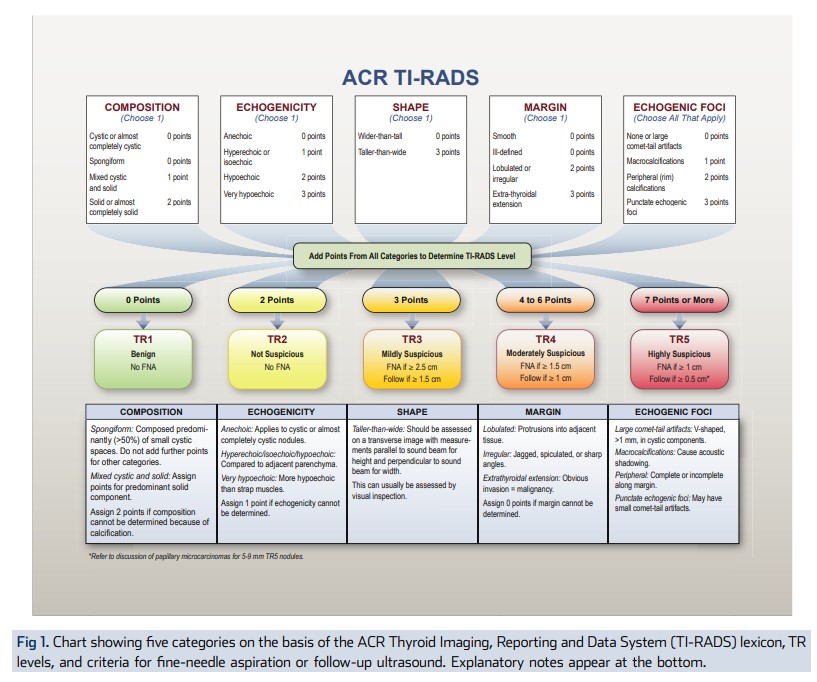
The ultrasound features in the ACR TI-RADS are categorized as benign, minimally suspicious, moderately suspicious, or highly suspicious for malignancy. Points are given for all the ultrasound features in a nodule, with more suspicious features being awarded additional points. Figure 1 presents these features arranged per the five lexicon categories [8]. When assessing a nodule, the reader selects one feature from each of the first four categories and all the features that apply from the final category and sums the points. The point total determines the nodule’s ACR TI-RADS level, which ranges from TR1 (benign) to TR5 (high suspicion of malignancy). Note that although it is possible for a nodule to be awarded zero points and hence be characterized as TR1, all other nodules merit at least two points because a nodule that has a mixed cystic and solid composition (one point) will also gain at least one more point for the echogenicity of its solid component. Finally, although sonoelastography is a promising technique [20, 21], it is probably not available in many ultrasound laboratories and is not incorporated into the ACR TI-RADS.
TAKE-HOME POINTS
– The goal of this project is to define a risk stratification system for thyroid nodules (ACR TI-RADS) to guide decisions regarding FNA and follow-up.
– The ACR TI-RADS chart allows practitioners to
assign points to nodules based on ultrasound features from a standardized lexicon that lends itself to structured reporting.
– The features that form the basis of this system will be assessed for inter-observer variability in a parallel project.