
The Curbsiders Internal Medicine Podcasts are outstanding. And Episode #67: Chronic Kidney Disease Pearls with @kidney_boy, Joel Topf [Link is to the show notes and podcast] NOVEMBER 13, 2017 is a great resource. I went ahead and embedded the podcast so I can easily relisten to it easily.
The show notes are as always incredible and so you’ll want to review them after you listen to the podcast.
Dr. Topf recommends that we obtain a spot urine protein/creatinine ratio in the evaluation of mild kidney failure in addition to a spot albumin/creatinine ratio. The reason is that multiple myeloma, a not infrequent cause of kidney failure, can only be diagnosed by urinary protein which includes the measurement of albumin and globulins.
Dr. Topf first discusses his approach to a patient, a 56 yo African-American, with a serum creatinine of 1.7 which his baseline. The patient has heart failure, diabetes, hypertension, and CKD. He hasn’t been to the doctor in a long time (he just got his insurance back) so he’s a new patient to the clinic. He is not on any medicines. His creatinine is found to be 1.7
Dr. Topf estimates the GFR using the CKD-EPI CREATININE EQUATION (2009) [Link is to the formula and explanation page of the National Kidney Foundation]. And here is a link to the calculator CKD-EPI Equations for Glomerular Filtration Rate (GFR) Estimates GFR based on serum creatinine, serum cystatin C, or both from MDCalc.
Dr. Topf says that:
Transcribe the speech starting at 9:37
Dr. Topf’s estimate of the above patient’s GFR using the CKD-EPI is
Here are excerpts from the show notes [See the episode’s time stamps in Resources at the end of the episode]:
- What equation should be used to estimate GFR? CKD-Epi. Based on largest population of any calculator. Best for “normal sized people.”
- 24 hour urine creatinine clearance equation works for all patients regardless of size e.g. bodybuilder, or amputee. Can be corrected for body surface area (click link) [Urine Cr (mg/dl) * Urine volume (ml)] / [Plasma Cr (mg/dl) * Time (min)] = CrCl
- How does age affect GFR? Controversial – adults are expected to lose approximately 1 ml/year of GFR past age 40.
- Recommended workup for new diagnosis of CKD:
- Urinalysis: Quantify proteinuria
- Diabetic nephropathy gradually increases proteinuria (takes years)
- Glomerulonephritis rapidly increases proteinuria
- Urine Albumin-to-creatinine misses multiple myeloma Bence-Jones proteins; instead useprotein-to-creatinine ratio.
- Urine dipstick only tests for albumin, not globulin fraction of protein
- Consider biopsy if significant proteinuria and no history of diabetes
- Ultrasound: A low yield test but may catch treatable problems e.g. athlerosclerotic disease, tumor, obstruction
- Recommended workup for new diagnosis of CKD:
- Urinalysis: Quantify proteinuria
- Diabetic nephropathy gradually increases proteinuria (takes years)
- Glomerulonephritis rapidly increases proteinuria
- Urine Albumin-to-creatinine misses multiple myeloma Bence-Jones proteins; instead useprotein-to-creatinine ratio.
- Urine dipstick only tests for albumin, not globulin fraction of protein
- Consider biopsy if significant proteinuria and no history of diabetes
- Ultrasound: A low yield test but may catch treatable problems e.g. athlerosclerotic disease, tumor, obstruction.
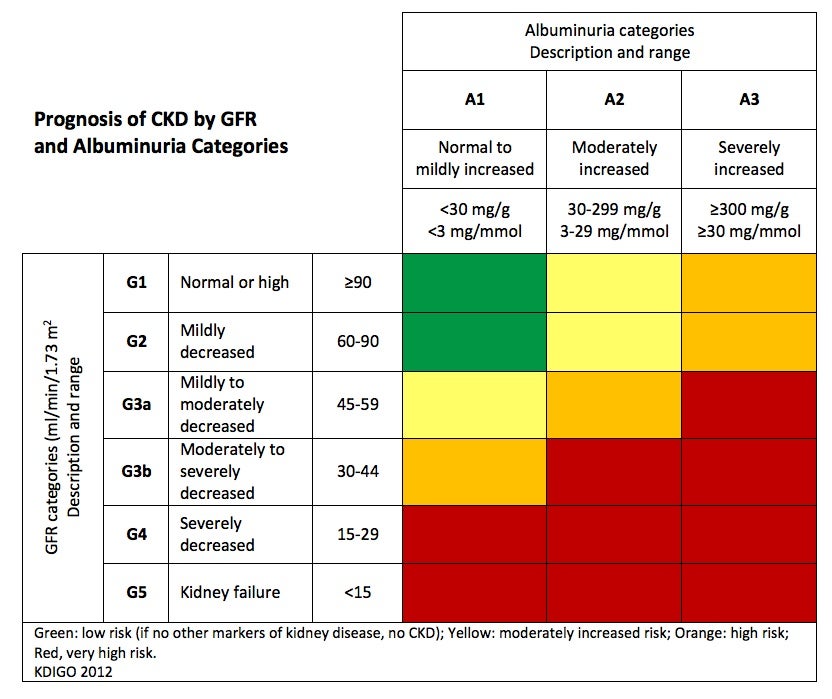
- Staging of CKD
- Kidney Heatmap for Staging
- Kidney Failure Risk calculator (estimated 2 and 5 year risk of needed dialysis)
Based on Tangri et al, JAMA 2016- Refer patients if:
- You feel uncomfortable
- Persistent hematuria
- eGFR < 30
- Significant proteinuria (>2gm/day)
- Uncontrolled hypertension
Resources:
Time Stamps
- 00:00 Intro
- 03:13 Pick of the weeks
- 08:49 Clinical Case
- 09:36 How to explain CKD to patients
- 12:16 Loss of GFR with age
- 13:22 Which equation should be used to estimate GFR
- 18:05 Creatinine clearance from 24 hour urine collection
- 22:25 Initial workup upon diagnosis of CKD
- 25:40 Interpreting tests for proteinuria
- 26:52 Staging and prognosis in CKD
- 32:00 Completing the initial workup for CKD
- 33:52 Who needs a referral to nephrology?
- 35:53 What labs to check in CKD and a discussion of secondary hyperparathyroidism
- 40:32 Take home points
- 42:30 Outro




{kind=link}