
Note to readers: I excerpt from my study materials because it helps me retain the material (sort of like highlighting in the old, pre-computer, days). You should just go to the podcast and show notes linked below. As my excerpts are not complete.
In this post I link to and excerpt from Emergency Medicine Cases‘ Ep 153 Pediatric Minor Head Injury and Concussion. Podcast production, sound design & editing by Anton Helman. Written Summary and blog post by Winny Li, edited by Anton Helman March, 2021.
All that follows is from the above show notes:
We see about 750,000 pediatric patients annually with traumatic head injury in EDs across North America. That’s a lot of kids. While most of these kids will be fine regardless of what we do in the ED, even minor pediatric head injury may require neurosurgical intervention, investigating is not without serious risk, there may be long term consequences even with trivial bonks and the signs can be devilishly subtle. Recent literature suggests that pediatric patients take longer to recover from mild traumatic brain injury compared to adults and persistent post-concussive symptoms (PPCS) after 1 month occur in up to 30% of children after minor head injury. These children can and should be identified in the ED based on the PPCS clinical risk score. In this EM Cases main episode podcast “Pediatric Minor Head Injury and Concussion” Dr. Sarah Reid and Dr. Roger Zemek discuss how best to incorporate the PECARN and CRASH2 decision tools into your practice, the role of Fast MRI, how to identify children who are at risk for long term sequelae after a minor head injury and how to manage persistent concussion symptoms when a child returns to the ED after a minor head injury….
Classification of pediatric head injury
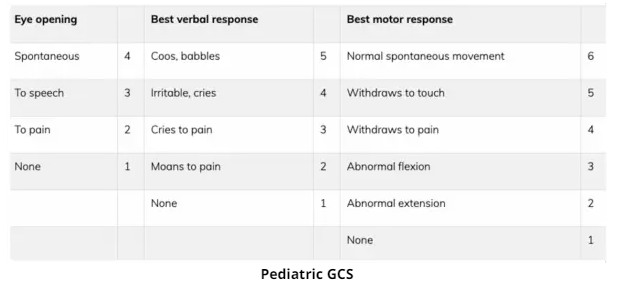
The classification of pediatric head trauma is divided into minor, moderate and severe which are defined by GCS cut offs on first assessment in the ED.
GCS 14 to 15: Minor head trauma
GCS 9 to 13: Moderate head trauma
GCS ≤8: Severe head trauma
Minor head injury is defined as injury within the past 24 hours associated with one of the following:
- Witnessed loss of consciousness
- Definite amnesia
- Witnessed disorientation
- persistent vomiting (> 1 episode) or
- persistent irritability (< 2 years old)
- and a GCS score of 14–15
Fortunately, only 5% of children with minor head injury will have an intracranial abnormality and about 1% will have a clinically important outcome. It is important that we use our history and physical exam to identify the patients at high risk for a clinically important outcome.
Key features on history to identify children at risk for an intracranial lesion requiring imaging
Mechanism of injury
PECARN: severe mechanism (MVC with ejection, death another passenger, rollover, pedestrian or bicyclist w/o helmet struck by motorized vehicle, fall 0.9m or 3ft, head struck by high-impact object)
CATCH2: high risk mechanism (fall ≥3ft or 5 stairs, bicycle with no helmet), worsening headache, persistent irritability if under 2 years old)
Recurrent vomiting
Isolated vomiting in the absence of other high-risk factors is rarely associated with significant traumatic brain injury (TBI). Recurrent vomiting (≥ 4 episodes, at least 15min apart) is a significant risk factor for intracranial injury in children after minor head injury. The addition of ≥ 4 episodes of vomiting to CATCH2 increased sensitivity to 100% for neurosurgical intervention and 99.5% for any brain abnormality.
Age and persistent irritability
Not acting normally as per parent or persistent irritability is always a worrisome sign in a head-injured child under the age of 2 years. In a nonverbal child, assess whether the child can be settled by their caregiver.
CT should be more strongly considered for children with multiple findings, worsening symptoms or signs, and for infants younger than 3 months of age – owing to their limited ability to communicate and thinner skull.
Isolated features on history not associated with an intracranial lesion requiring imaging
Children who present with the following isolated clinical features with no high risk features on history or physical have an extremely low risk of clinically important TBI and can generally be safely discharged without imaging:
- Isolated headache
- Isolated loss of consciousness (LOC)
- Impact seizure (seizure immediately following head injury)
Key physical exam findings/maneuvers to identify children at risk of intracranial injury or post-concussion symptoms
Assess the child’s general appearance, GCS (see below), mental status and whether they are agitated, somnolent, displaying repetitive questioning or are slow to respond. Look for signs of basal skull fracture including hemotympanum, Battle’s sign, raccoon eyes, and CSF rhinorrhea. Palpate to look for a skull fracture and for non-frontal boggy scalp hematoma >2cm in size, which carries a higher risk for clinically important outcomes.
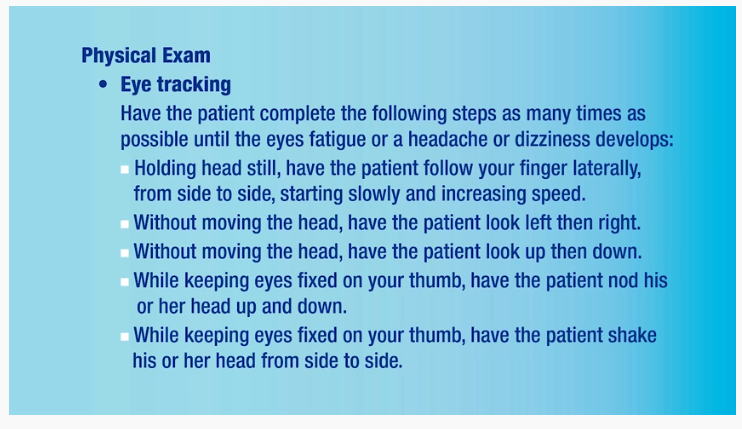
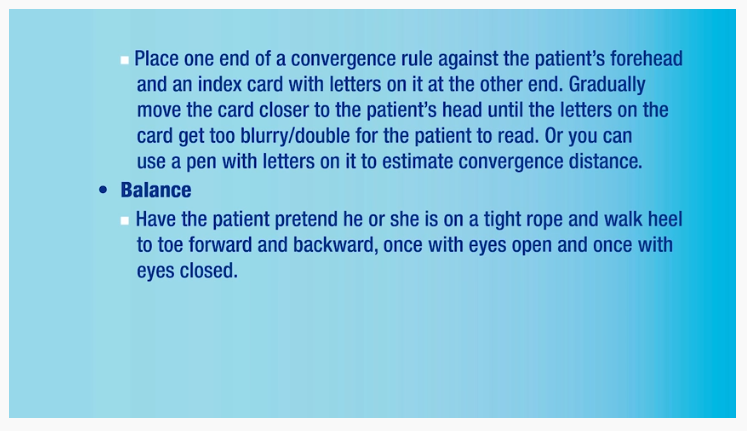
Vestibular and oculomotor screening (VOMS) examination for concussion
In addition to the screening neurological examination to evaluate for an intracranial lesion, evaluate for vestibular and oculomotor dysfunction, which has a high predictive value in identifying concussion and aids in prognostication for persistent concussion symptoms.
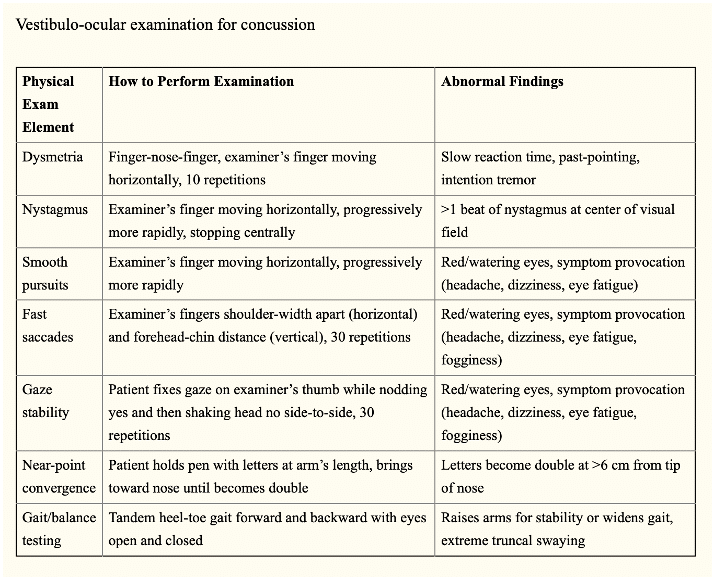
The video below demonstrates in clear concise manner all of the maneuvers in the above table.
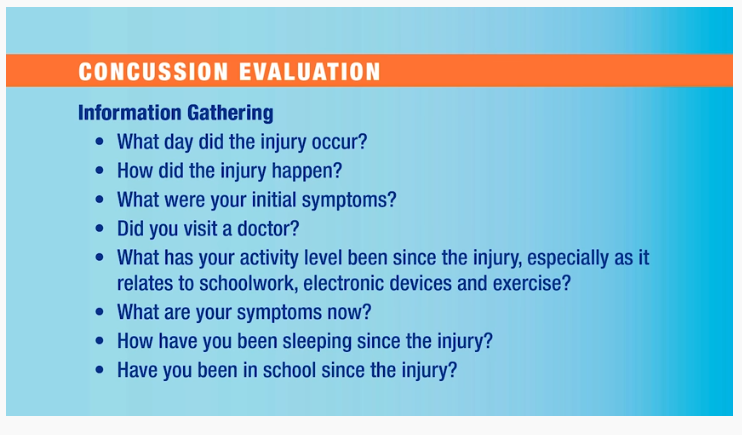
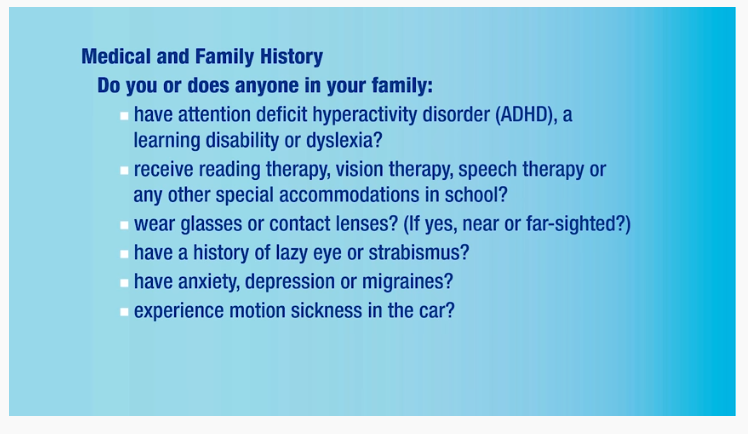
Pediatric Exams: Concussion Evaluation
May 19, 2015Video demonstrating modified vestibulo-ocular exam for concussion (minutes 3:13-6:03)
I’ve included the following slides from the above video:
Returning now to excerpts from Ep 153 Pediatric Minor Head Injury and Concussion:
Pediatric head injury decision tools: PECARN and CATCH2 – which to use and when?
Pediatric head injury decision rules were developed to decrease CT utilization and radiation effects of CT. In counselling parents, comparison to background radiation dose may be helpful: in comparison to a CXR which has a similar radiation dose to ~10 days of background radiation for a child, a CT head has a similar radiation dose to ~8 months of background radiation.
PECARN
US-based study, where the baseline assumption was that everyone needed a scan, thus the rule was developed in order to determine who doesnot need a CT scan.
Note that regardless of age group, PECARN recommends a CT scan in any child who presents with a Glasgow Coma Scale < 15, altered mental status, signs of palpable or basilar skull fracture. It included patients with GCS of 14-15.
CATCH2
Canadian study, and the baseline assumption was that no one needed a scan (as to prevent radiation risk), thus rule was developed to determine who doesneed a scan. It included patients with GCS of 13-15.
The original CATCH study had a sensitivity of 91% for neurosurgical intervention, but the addition of “>4 episodes of vomiting” resulted in a refined 8-item rule (CATCH2) with 100% sensitivity for neurosurgical intervention and 99.5% sensitivity for brain injury.
CATCH on MDcalc (note that CATCH2 requires “>4 episodes of vomiting” in addition to CATCH)
Bottom line: Our experts recommend using PECARN in patients with GCS 14-15 in whom your gestalt is that they do not require a CT scan and using CATCH2 in patients with a GCS of 13 in whom your gestalt is that they do require a CT scan.
Role for Fast-MRI as an initial imaging modality in minor head injury
In one small study, Fast MRI had a sensitivity of 92.8%, missing isolated skull fractures and small subarachnoid hemorrhage that did not require neurosurgical intervention. While larger studies are required, Fast MRI has potential as a radiation-sparing imaging modality for pediatric head injury in centers with quick access to MRI and radiologist experience with the modality for this specific indication.
Observation of the child with minor head injury and concussion in the ED
Many patients who are assessed using the PECARN tool require a period of observation and reassessment to identify evolving high risk features requiring imaging. Although an optimal duration of ED observation after minor head injury remains to be determined, a large retrospective study of children <14 years of age with minor head trauma demonstrated that only 5% of children were diagnosed with ICH more than 6 hours after the time of injury. Therefore, the necessary ED observation length is likely no more than 6 hours from the time of injury and is reasonable to consider active observation at home with appropriate caregiver instruction.
Concussion diagnosis, discharge instructions and follow up
Most children with concussion recover within 2 weeks, however persistent post-concussive symptoms (PPCS) after 1 month occur in up to 30% of children after minor head injury. Thus, in the ED, it is important to identify these children and set expectations for possible PPCS and follow-up of the above-mentioned delayed symptoms. Furthermore, there is evidence that pediatric patients take longer to recover from mild traumatic brain injury compared to adults.
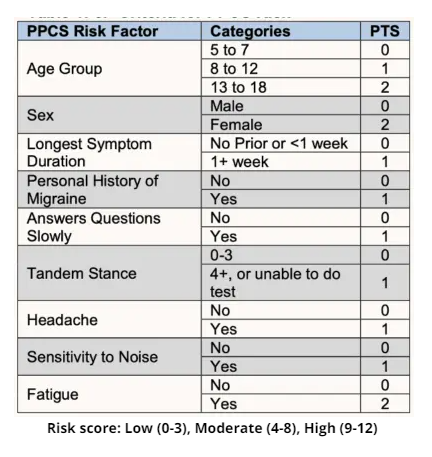
Our experts recommend using the PPCS clinical risk score for predicting risk of post-concussive symptoms. The tool performed significantly better than physician judgment in predicting PPCS. Consider early referral to a multidisciplinary head injury team for children with prolonged concussion symptoms or those at high risk for having prolonged symptoms as per the PPCS clinical risk score.
Discharge instructions for pediatric minor head injury and concussion
Cognitive rest after minor head injury and concussion
Most children require a 24-48 hour break from school followed by gradual return to full academic/cognitive activities. Prolonged rest beyond the first 24-48 hours after a concussion is no longer recommended and may be associated with harm.
Parental advice on “screen” time: AAP recognizes that young adults are highly connected through social media and electronics. Removing them may result in feelings of anxiety and isolation. Thus hand-held devices and video games should be limited in patients with particular light sensitivity or oculomotor dysfunction, but otherwise the conservative use of electronics seems to be harmless.
Physical rest after minor head injury and concussion
An initial period of 24-48 hours of rest is recommended before starting a graduated return to physical activity. Patients may begin light physical activity even if symptoms are present as long as symptoms are tolerated.
Children and adolescents should return to a full school load, without accommodation, before they return to full-contact sport and game play.
Parachute Canada Concussion protocols (Return to school/play/work)
Sleep hygiene and adequate hydration have been suggested as important aspects of treatment after minor head injury.
Take home points for pediatric minor head injury and concussion
- Minor head injury is defined as injury with one of the following: witnessed LOC, amnesia, disorientation, persistent vomiting (>1 episode), persistent irritability (<2years old) and GCS 14-15
- High risk features on history to help identify children at risk of intracranial injury include: severe mechanism of injury as per PECARN and CATCH2, recurrent vomiting >4 episodes, worsening headache, persistent irritability under the age of 2, and delayed post-traumatic seizure
- Isolated features on history that are not associated with clinically important TBI include: isolated headache, isolated loss of consciousness and isolated impact seizure
- On physical exam, examine for a non-frontal boggy scalp hematoma >2cm as this is a high risk feature for skull fracture and TBI requiring neurosurgical intervention
- Routinely evaluate for vestibular and oculomotor dysfunction, which may help identify concussed patients as well as prognosticate those at risk for prolonged recovery from concussion
- PECARN was developed in order to determine which patients do not require a CT scan
- CATCH was developed in order to determine which patients do require a CT scan. CATCH2 included “>4 episodes of vomiting” with 100% sensitivity for neurosurgical intervention and 99.5% sensitivity for brain injury
- POCUS can be useful in the ED to assist in diagnosing skull fractures and inform next investigative steps
- Consider Fast MRI if available in your ED as an alternative to CT for high risk minor head injury patients in which there is a concern for radiation exposure, understanding that it may miss skull fractures and small subarachnoid hemorrhages
- If observation in the ED is required as per the PECARN tool, the necessary observation length has not been definitely defined, however it is likely no more than 6 hours from the time of injury
- Children take longer to recover from TBI compared to adults, and 30% have persistent symptoms at 1-month
- Use the Persistent Post-Concussive Symptoms (PPCS) Risk score to identify those at high risk and consider early referral to multidisciplinary services
- The mainstay of concussion treatment is a short period of physical and cognitive rest (24-48hrs) followed by gradual return to activities
Additional resources
Ontario Neurotrauma foundation (ONF): https://onf.org/knowledge-mobilization/acquired-brain-injury/guidelines-for-concussion-and-moderate-to-severe-traumatic-brain-injury/
Brain Injury Guidelines: https://braininjuryguidelines.org/
5P Calculator: https://www.5pconcussion.com/en/scorecalculator
CATT – concussion assessment training tool: https://cattonline.com/
Parachute Canada Concussion protocols (Return to school/play/work): https://parachute.ca/en/professional-resource/concussion-collection/concussion-protocol-resources-for-schools/



