Today, I review, link to, and embed Postadenoidectomy hemorrhage: how we do it?, from Int J Clin Exp Med. 2015 Feb 15;8(2):2799–2803. Nevzat Demirbilek 1, Cenk Evren 1, Uzay Altun 1. PMCID: PMC4402885 PMID: 25932238.
All that follows is from the above resource.
Abstract
Aims: Conventionally, adenoidectomy has been performed using blind curettage. Postoperative hemorrhage is the most common complication of surgery. There is no specific management algorithm in the literature. In this study, we described an endoscopic approach in the management of postadenoidectomy hemorrhage. Material and methods: Between 1995 and 2014, 7946 patients undergoing adenoidectomy under general anesthesia in our clinic were retrospectively analyzed. All patients had a rest adenoid tissue located in the choanae. Endoscopic excision of the tissue was performed without using a post-nasal pack. Results: All patients (100%) had a rest adenoid tissue located in the choanae. Hemorrhage was completely discontinued with endoscopic excision of the hemorrhagic tissue. Conclusion: Based on our study findings, we conclude that an endoscopic approach should be applied in all postoperative patients with hemorrhage who are unresponsive to conservative treatment modalities.
Keywords: Adenoidectomy, hemorrhage, complication, endoscopy, postoperative Introduction
Adenoidectomy is one of the most frequent operations in pediatric population [1]. The main indications include obstructive sleep apnea, recurrent otitis media, otitis media with effusion, sinusitis, and recurrent adenotonsillitis [2,3]. The adenoid is located in the midline of the posterior nasopharyngeal wall immediately below the rostrum of the sphenoid. Surgical exposure and approach to this region are extremely challenging [4]. Conventionally, adenoidectomy has been performed using blind curettage [4]. In another words, the surgeon does not see but perform surgery with the guidance of an adenotome. Hence, the rate of postoperative recurrence and associated treatment failure is highly increased than anticipated. Hemorrhage is the most severe complication of adenoidectomy [3,4]. There are a number of studies describing various surgical techniques, duration of surgery, and the amount of intraoperative blood lost in the literature [1,5–9]. However, a limited number of reports on possible risk factors for postadenoidectomy hemorrhage and management strategies is available [3,4,10,11]. Herein, we describe an endoscopic approach in the management of postadenoidectomy hemorrhage, although rare, which may be comfortable for both the surgeon and patient in the light of literature data.
Materials and methods
Between 1995 and 2014, 7946 patients undergoing adenoidectomy in our clinic were retrospectively analyzed.
Adenoidectomy was performed in Rose or head hanging position under general anesthesia with oral endotracheal intubation. The posterior and lateral nasopharyngeal walls were palpated. A nasopharyngeal mirror was used to visualize the nasopharynx and to guide the surgical dissection. Conventional curettage was performed using the Beckmann adenotome. At the end of the procedure, a pack of gauze was inserted into the nasopharynx for a few minutes. Curettage was repeated in the presence of a rest tissue or electrocautery-based management was administered in patients suffering from hemorrhage. Of note, spontaneously discontinued anterior or posterior minimal leaks were excluded.
Surgical technique
All patients were instructed to rinse their mouth with cold epinephrine-containing solution and intravenous fluid was administered. Pulse and blood pressure were monitored hourly and hematocrit values were observed. The patients with an active or post-nasal hemorrhage with reduced hematocrit values were operated under general anesthesia. Initially, a pack of gauze was inserted into the hypopharynx. The head was elevated at a 30° angle. Decongestion was maintained through epinephrine nasal packing. A 0-degree endoscope was used to visualize nasopharynx and hemorrhage site. Endoscopic excision of the hemorrhagic tissue was safely performed through a punch. Hemorrhage was completely discontinued without requiring electrocauterization or post-nasal packing.
Results
Adenoidectomy was performed in combination with tonsillectomy in 53% of patients. A total of 7931 were children (mean age: 45 months; range 24 months to 13 years) and 15 were adults (mean age: 25 years; range 18 to 31 years).*
*The Diagnostic Value of CT Scan in Identifying Adenoid Hypertrophy in Adults: A Case Report [PubMed] [Full-Text HTML] [Full-Text PDF]. Cureus. 2024 Jun 20;16(6):e62793. doi: 10.7759/cureus.62793. eCollection 2024 Jun.
Four patients (0.05%) had postoperative hemorrhage including one at three hours, two at five days, and the other at 18 days. During baseline screening, hemorrhage was managed in three patients who underwent conventional adenoidectomy in other healthcare facilities. All three patients had hemorrhage in the second postoperative day. Of a total of seven patients with postoperative hemorrhage, three were girls and four were boys (mean age: 40 months; range 36 months to 9 years). Isolated adenoidectomy and adenoidectomy combined with tonsillectomy were performed in five and two patients, respectively.

Nasal Cavity. Anatomy of the nasal cavity, including the frontal sinus, superior turbinate, middle turbinate, inferior turbinate, sphenoid sinus, nasopharynx, adenoid pad, eustachian tube orifice, fossa of Rosenmuller, and nasal vestibule. Contributed by B Palmer
From: Anatomy, Head and Neck, Nasal Cavity
Treasure Island (FL): StatPearls Publishing; 2025 Jan-.
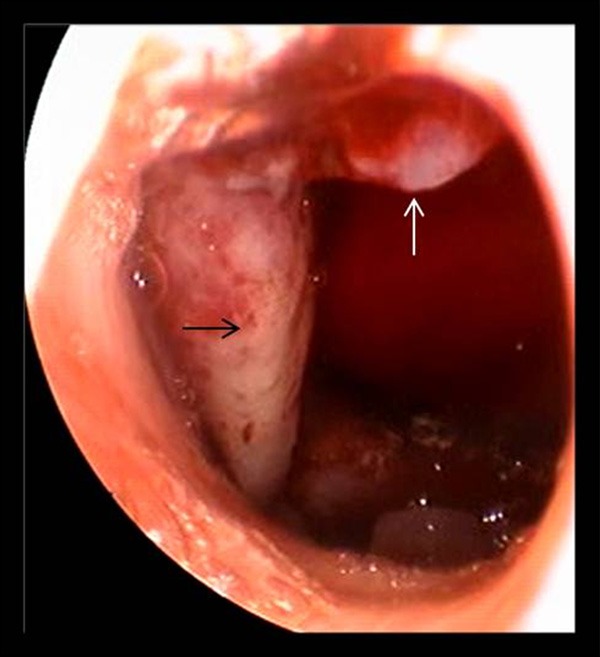
All patients (100%) had a rest adenoid tissue located in the choanae (Figure 1). Pathological examination results were reported as lymphoid hyperplasia in all patients. None of the patients had preoperative coagulation disorder. One patient with low hemoglobin level (8 g/dL) received a unit of erythrocyte suspension. No ligated external carotid artery or death events were reported during 19-year follow-up.
Figure 1
White arrow: Hemorrhagic adenoid tissue of the choanae. Black arrow: Torus tubarius.
Discussion
Conventional adenoidectomy is a simple and rapid surgical procedure which is performed by adenoid curettage with a transoral indirect mirror or headlight [12,13]. The procedure has been performed for many years [6,9]. Visualization can be maintained through palpation or a nasopharyngeal mirror. Telescopes inserted through the oropharynx or nose can be also helpful in uncommon cases [14]. The main disadvantage of this procedure is the presence of a rest tissue after surgery as well as damage to the nasopharyngeal mucosa and torus tubarius [3,8].
In this present study, we performed adenoidectomy using a nasopharyngeal mirror which partly failed to visualize intraoperative hemorrhage and tissue edema in the choanae, in particular. We, therefore, recommend endoscopic inspection, if available. This may result in decreased postoperative hemorrhage and increased removal of residual tissue.
Postoperative hemorrhage is the most common complication of adenoidectomy with a life-threatening potential [3]. Postadenoidectomy hemorrhage can be fatal. The incidence of postadenoidectomy hemorrhage is 0 to 0.49% in the literature [18–20].
Tomkinson et al. [10] compared demographic characteristics of the patients with postoperative hemorrhage. These included age and sex of the patients, surgical technique, and surgeon’s experience. The authors found no specific risk factors. Twenty two patients (0.39%) had postoperative hemorrhage in the adenoid bed required re-do surgery within the first 24 hours. None of the patients had severe hemorrhage after the first 24 hours. Only eight patients (0.07%) had mild hemorrhage which spontaneously resolved.
In case of postadenoidectomy hemorrhage, blind oral palpation mostly fails to detect the rest tissue. It is usually infeasible to detect the exact site of blood pooling using a mirror in the Rose position (head hyperextension) or using a 30 to 70° endoscope. Based on our clinical observation, we suggest that this position may complicate the detection of the hemorrhage site. Therefore, the head was elevated at a 30° angle in our study, as in the ear nose throat surgery practice.
A recent study of posttonsillectomy and postadenoidectomy hemorrhage have confirmed that adenoidectomy has a considerably lower hemorrhage rate than tonsillectomy [3]. Unlike posttonsillectomy hemorrhage, cold solutions for mouthwash are not effective for postadenoidectomy hemorrhage, as the adenoids are located behind the nasal cavity. The literature data recommends re-curettage, cauterization or posterior nasal packing [4,10,11,19]. In addition, post-nasal packs are considered effective for achieving hemostasis [2,10]. In a study conducted in England, a total of 87% of ENT surgeons were reported to manage primary hemorrhage with post-nasal packs, while 78% used an overnight post-nasal pack [11]. Furthermore, Tzifa et al. [11] reported that post-nasal packing for four hours would be helpful to manage early postoperative hemorrhage. In a study including 1051 patients undergoing conventional adenoidectomy, Milosevic [3] performed general anesthesia in two patients (0.19%) due to serious hemorrhage within the first nine hours of surgery and post-nasal packs were placed. As in the present study mainly including young children, post-nasal packing under local anesthesia is not feasible. The patients should be hospitalized, until the nasal pack is removed. Time to removal is challenging for both patients and their parents. Post-nasal packing are also associated with various side effects such as hypoxia, respiratory obstruction, infection, sepsis, and toxic shock [21,22]. In addition, recurrent tissues cannot be removed by posterior nasal packing. In the absence of hemorrhagic diathesis, the rest adenoid is the most frequent cause of postoperative hemorrhage [3,4,20]. Similarly, the origin of the postadenoidectomy hemorrhage was the rest tissue in the choanae in all cases in our study. We did not use post-nasal packs. We believe that hemorrhagic events may relapse, unless the rest tissue is removed.
Moreover, nasopharyngeal stenosis is another rare complication of adenoidectomy. Erosion of the deep tissues through over cauterization may increase the risk of the complication [23]. Therefore, we did not perform electrocauterization or re-curettage in our patients with postoperative hemorrhage to avoid any damage to the deep tissues. None of the patients had stenosis during one year follow-up.
Review of the literature shows that surgery under direct visualization produces a lower rate of postoperative hemorrhage. In an adenoidectomy study using a microdebrider as an endoscopic tool, Somani et al. [1] reported no postoperative hemorrhage or recurrence. However, the authors reported some disadvantages: surgical technique requiring expensive equipment and the difficulty in maneuvering the microdebrider tip into the nasopharynx. In another study, Costantini et al. [8] performed adenoidectomy using a microdebrider and reported that one of 201 patients had hemorrhage in the fourth postoperative day, which spontaneously resolved. No recurrence was observed in the study population.
Conclusion
In conclusion, postadenoidectomy hemorrhage is an unlikely complication for both the patient and surgeon. Based on the literature data, we conclude that the rate of postoperative hemorrhage is higher in patients undergoing curettage than endoscopic inspection. Although we used a mirror during surgery, we recommend endoscopic inspection during surgery to prevent this undesirable complication, if available. We believe that it would be not possible to thoroughly view the choanae with a mirror for possible hemorrhagic events or tissue edema. Therefore, we suggest that this complication can be successfully managed by endoscopic.