In addition to today’s resource please review this link to the American College of Rheumatology‘s Clinical Practice Guidelines:
- Axial Spondyloarthritis
- Glucocorticoid-Induced Osteoporosis Guideline
- Gout Guideline
- Integrative RA Treatment Guideline
- Interstitial Lung Disease Guideline
- Juvenile Idiopathic Arthritis Guideline
- Lupus Guideline
- Lyme Disease Guideline
- Optimal Timing of Total Hip and Knee Arthroplasty
- Osteoarthritis Guideline
- Perioperative Management Guideline
- Polymyalgia Rheumatica Guideline
- Psoriatic Arthritis Guideline
- Reproductive Health in Rheumatic Diseases Guideline
- Rheumatoid Arthritis Guideline
- Vaccinations Guideline
- Vasculitis Guideline
Today, I review, link to, and excerpt from Practical Use of Ultrasound in Modern Rheumatology—From A to Z [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. by Tanya Sapundzhieva 1,2 ORCID,Lyubomir Sapundzhiev 1,2 ORCID andAnastas Batalov 1,3.
There are 101 similar articles in PubMed.
The above article is cited by two articles in PubMed.
All that follows is from the above resource.
Abstract
During the past 20 years, the use of ultrasound (US) in rheumatology has increased tremendously, and has become a valuable tool in rheumatologists’ hands, not only for assessment of musculoskeletal structures like joints and peri-articular tissues, but also for evaluation of nerves, vessels, lungs, and skin, as well as for increasing the accuracy in a number of US-guided aspirations and injections. The US is currently used as the imaging method of choice for establishing an early diagnosis, assessing disease activity, monitoring treatment efficacy, and assessing the remission state of inflammatory joint diseases. It is also used as a complementary tool for the assessment of patients with degenerative joint diseases like osteoarthritis, and in the detection of crystal deposits for establishing the diagnosis of metabolic arthropathies (gout, calcium pyrophosphate deposition disease). The US has an added value in the diagnostic process of polymyalgia rheumatica and giant-cell arteritis, and is currently included in the classification criteria. A novel use of US in the assessment of the skin and lung involvement in connective tissue diseases has the potential to replace more expensive and risky imaging modalities. This narrative review will take a close look at the most recent evidence-based data regarding the use of US in the big spectrum of rheumatic diseases.Keywords:ultrasound; rheumatology; musculoskeletal; imaging
1. Introduction
The first published data regarding the use of ultrasound (US) in rheumatology were in the late 1990s, when radiologists performed US examination to differentiate thrombophlebitis from a Baker’s cyst [1]. A few years after this report, the US image of synovitis in rheumatoid arthritis was described again by radiologists [2]. Initially, the US was mostly used for assessment of the large joints. With the technological advances and implementation of high-frequency transducers in the rheumatology practice, the number of published studies about the use of US for assessment of small joints has rapidly increased during the past two decades [3]. The increasing use of US in rheumatology is mostly due to the numerous advantages this imaging technique possesses, namely the lack of ionizing radiation, the cost effectivity, the possibility for simultaneous assessment of many structures and for dynamic evaluation of the area of interest, and the fact that it is patient-friendly and enables a more accurate and less risky performance of a number of joint and periarticular diagnostic and therapeutic procedures [3].The aim of this narrative review is to present in a clear and structured way the recent advances of US in rheumatology practice.2. US in Inflammatory Joint Diseases
2.1. US for Establishing a Diagnosis
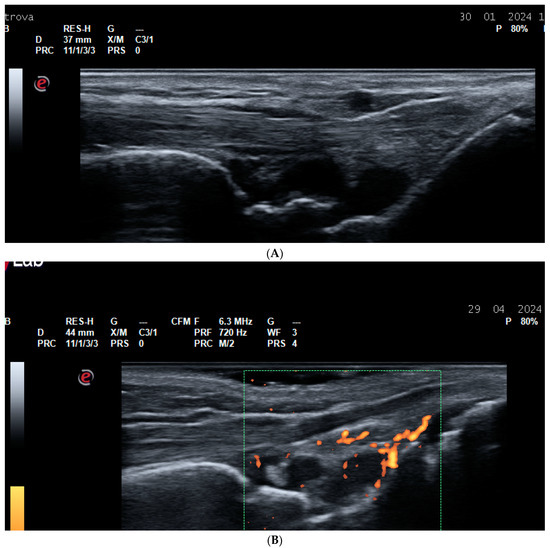
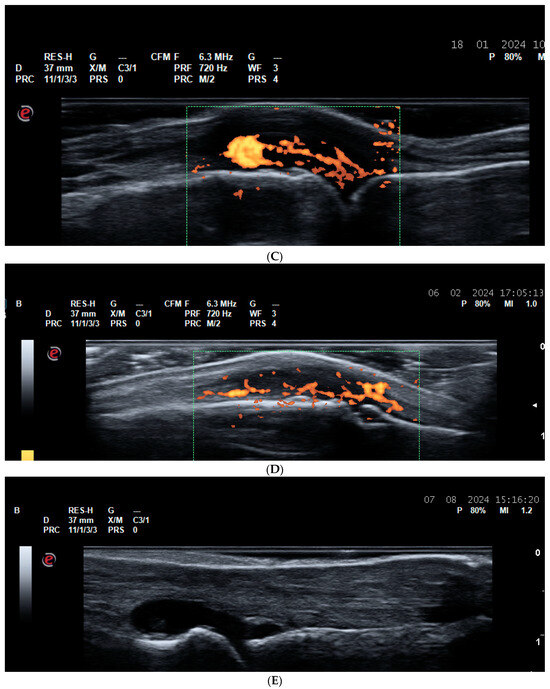
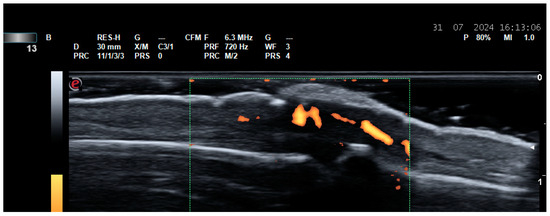
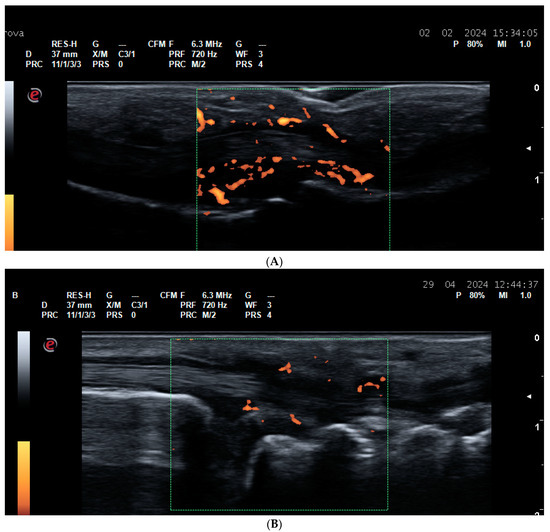
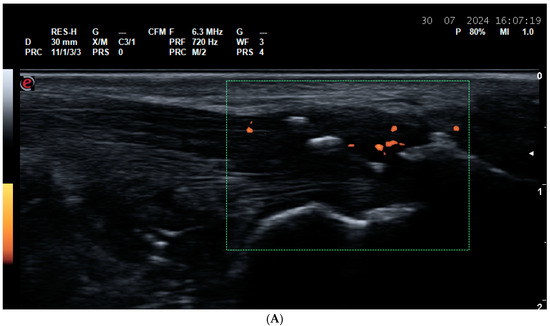
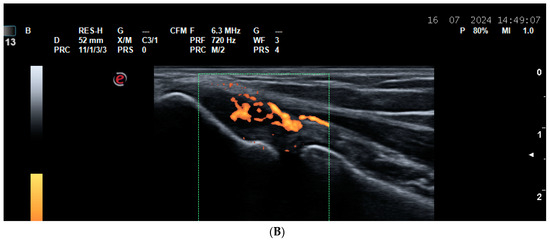
The US has been proven to be far more sensitive than the physical examination for the detection of synovitis, tenosynovitis, and enthesitis, thus being helpful in the establishment of early diagnosis of rheumatoid arthritis (RA) and spondyloarthritis (SpA) [4]. Please see Figure 1, Figure 2, Figure 3 and Figure 4. Subclinical synovitis and enthesitis is a common finding in the early stage of inflammatory joint diseases [4]. Therefore, the use of US in patients presenting with a new-onset inflammatory type of joint pain is of crucial importance in order not to delay diagnosis [4]. The number of US-detected inflamed joints and entheses has been proven to be greater than the number of inflamed joints/entheses found during physical examination [5,6,7,8,9,10].Figure 1. Synovitis. (A) A dorsal longitudinal scan of the wrist joint on Gray Scale Ultrasound (GSUS) in an RA patient—Grade 3 synovitis of the radiocarpal and intercarpal joints; (B) a dorsal longitudinal scan of the wrist joint on Power Doppler Ultrasound (PDUS) in an RA patient—Grade 2 synovitis; (C) a dorsal longitudinal scan of the second metacarpophalangeal (MCP) joint on PDUS in an RA patient—Grade 3 synovitis; (D) a dorsal longitudinal scan of the third proximal interphalangeal (PIP) joint on PDUS in an RA patient—Grade 3 synovitis; (E) a dorsal longitudinal scan of the first metatarsophalangeal (MTP) joint on GSUS—effusion and grade 3 synovitis.Figure 2. Paratenonitis—inflammation of the finger extensor tendon on PDUS. A dorsal longitudinal scan of the third PIP joint in a PsA patient.Figure 3. Tenosynovitis. (A) Finger flexor tenosynovitis—a palmar longitudinal scan of the second PIP joint in a PsA patient—Grade 3 tenosynovitis of the finger flexor tendon on PDUS; (B) tenosynovitis of the VI extensor compartment of the wrist—extensor carpi ulnaris tedon—in an RA patient—ulnar longitudinal scan—grade 2 tenosynovitis on PDUS; (C) tenosynovitis of the VI extensor compartment of the wrist—extensor carpi ulnaris in an RA patient—ulnar transverse scan—grade 2 tenosynovitis on PDUS.Figure 4. Enthesitis. (A) Enthesitis of the enthesis of the Achilles tendon on the calcaneus in a patient with ankylosing spondylitis. A thickened hypoechoic enthesis, with loss of the normal fibrillar pattern, calcifications, enthesophytes, exhibiting a PD signal; (B) enthesitis of the common extensor tendon enthesis on the lateral epicondyle of the humerus—thickened and hypoechoic enthesis, loss of the normal fibrillar pattern, exhibiting a PD signal.The US-detected subclinical synovitis has even been proven to be a predictor of developing arthritis in patients with arthralgia, and, vice versa, the absence of joint inflammation from the US assessment is a negative predictor [11,12,13,14].The US has even higher sensitivity than conventional radiography for the detection of structural damage, namely early erosions [15,16], and similarly to US-detected synovitis, US-detected erosions in arthralgia patients are also predictive of the development of arthritis [17,18].2.1.1. US in RA Diagnosis
The key elementary lesions detected by US in RA are synovitis, tenosynovitis, bursitis, erosions, synovial cysts, and rheumatoid nodules [4]. In patients with early RA, the number of inflamed joints and tendons assessed by US has been proven to be greater than the one assessed by physical examination, meaning that US can visualize subclinical inflammation; thus, patients previously considered to have oligoarthritis may be diagnosed with polyarthritis [4,5,6,19]. In 2019, a US multinational working group published definitions for the main lesions detected by US [20]. It is important to assess the synovial hypertrophy both on gray scale and on Power Doppler (PD) US, the latter providing valuable information for the activity of the synovitis [21].2.1.2. US in PsA Diagnosis
The inflammation of the entheses, termed enthesitis, along with synovitis, is considered to be the main inflammatory finding in patients with SpA, especially PsA [22,23]. Enthesitis has been documented to affect approximately 35% of PsA patients, being far more prevalent in PsA than in other joint diseases [24]. On the US, enthesitis presents with two types of lesions—inflammatory, consisting of the increased thickness of the enthesis, a hypoehogenic appearance, loss of the normal fibrillar pattern, and a positive PD signal, and structural, defined as the presence of enthesophytes, calcifications, or erosions at the entheseal level, considered to be no more than 2 mm distal to the tendon insertion on the bony surface [20]. According to the literature, the most commonly affected entheses in PsA are plantar fascia and Achilles tendon enthesis on the calcaneus, and the common extensor tendon enthesis on the lateral epicondyle of the humerus [24].The US reveals subclinical enthesitis, underlying the importance of screening with US the target entheses in PsA in patients with early arthritis [4,9,10].2.1.3. US Role for the Differential Diagnosis between RA and PsA
The US can be very helpful in the differential diagnosis between arthritides in the early stage, when clinical symptoms and physical findings may be similar, and specific disease-related features are still missing [25,26,27]. For example, the recognition of a specific pattern of inflammation by US can aid the rheumatologist to establish the correct diagnosis. Both RA and psoriatic arthritis (PsA) may present with symmetric involvement of the small joints of the hands. In the absence of specific erythematous papulous-squamous rash and specific antibodies, the early diagnosis can be challenging. The detection of mini-enthesitis by US is very specific for the diagnosis of PsA as compared to RA [25,28]. Mini-enthesitis encompasses several US-detected lesions, for example, inflammation of the paratenon of the finger extensor tendon (paratenonitis), inflammation of the small entheses of the central slip of the extensor tendon at the level of the proximal phalanx, or of the distal insertion at the distal phalanx, inflammation of the collateral ligaments of the small finger joints, inflammation of the pulley of the flexor tendon, and subcutaneous swelling around the finger flexor tendon (the so-called pseudotenosynovitis) [25].2.2. US for Assessment of Disease Activity and Monitoring Response to Therapy
In order to use the ‘treat-to-target’ strategy for the control of inflammation in inflammatory joint diseases, a number of studies recommend to use US to more accurately assess the disease activity state in addition to the clinical disease activity indices [29,30,31,32,33].The detailed US assessment of 28 joints is time consuming; therefore, a number of studies have been conducted exploring whether a reduced joint count is reliable enough to reflect disease activity and sensitive enough to reflect the therapeutic response. Currently, 7-, 8-, 9-, and 12-joint sets have been proven to correlate with the extensive and time-consuming US assessment of 24 or more joints [34,35,36,37].In addition to the role of US for assessing response to therapy in RA, a number of studies have used US to detect early treatment efficacy in PsA patients [38,39,40].Nevertheless, the results of two big randomized trials (the TASER and the ARCTIC) exploring the added value of US assessment of disease activity as compared to the classical assessment by composite clinical indices have revealed non-superiority of the imaging versus clinical evaluation for the treatment outcomes, thus highlighting the necessity for future studies to prove that US-based decision-making regarding management of patents with RA offers more benefits for the patient outcomes than clinical examination alone [41,42].2.3. US for Assessment of the State of True Remission
The purpose of treating RA is to reach remission because it is associated with the best functional and structural outcomes for the patients [43]. According to the latest European League Against Rheumatism (EULAR) recommendations for management of RA, rheumatologists should define remission based on two definitions—the Boolean or index-based American College of Rheumatology (ACR)-EULAR remission definition [44]. Nevertheless, a number of RA patients still experience radiographic progression despite being in a state of remission [45]. A possible explanation for this concordance is the fact that many patients in clinical remission have evidence of persistent PD positive synovitis seen on US [37,43,46,47]. The practical implication for defining which patients are in the state of deep remission (clinical and US) is the fact that the risk of a disease relapse after drug tapering is the smallest [48,49,50]. Thus, the US may help the rheumatologist to decide which of the patients in clinical remission are suitable for attempting to decrease the dose or increase the interval for biologic drug administration [49,50]. A systematic review and meta-analysis have proven that subclinical joint inflammation, detected by US, is a predictor for a future flare and structural progression in RA patients in remission according to the composite disease activity indices [51].After having discussed the role of US for the assessment of remission, the benefit of incorporating US in the management of patients with difficult-to-treat RA (D2T-RA) has also been proven [52]. In a recent study by David et al., US was used to distinguish different phenotypes of D2T RA patients—an inflammatory, characterized by US evidence of synovitis or tenosynovitis, versus a non-inflammatory [52]. The study shows that as many as 43% of D2T-RA do not to have evidence of joint or tendon inflammation and have higher prevalence of a high body mass index and fibromyalgia [52]. This finding has a practical implication; those patients would not benefit from escalation of therapy or switching to another drug class, as compared to the patients with the inflammatory phenotype, suggesting that in this clinical scenario, US-driven patient management may prove to be superior versus a clinically-driven strategy [52,53].