
I originally reviewed this post on May 19, 2025 but I am reviewing it again and moving it to 6-18-2025.
Today, I review, link to, and excerpt from The Curbsiders‘ #476 Medications for Alcohol Use Disorder 2.0 with Dr Stephen Holt. March 24, 2025 | By Shawn Cohen*
*Cohen SM, Holt SR, Sonoda K, Williams PN, Chan, CA. “#31 Medications for Alcohol Use Disorder 2.0”. The Curbsiders Addiction Medicine Podcast. https://thecurbsiders.com/addiction. March 24, 2025.
All that follows is from the above resource
.
Transcript available via YouTube
Make MAUD your topira-MATE
Level up your treatment for people with alcohol use disorder. Learn about medication options beyond the first line, when they’re appropriate and not, and how to work with your patients to set goals that fit them. We’re joined by Dr Stephen Holt (Yale University School of Medicine)
Claim CME for this episode at curbsiders.vcuhealth.org!
By listening to this episode and completing CME, this can be used to count towards the new DEA 8-hr requirement on substance use disorders education.
Episodes | Subscribe | Spotify | iTunes | CurbsidersAddictionMed@gmail.com | CME!
Production Partner: Providers Clinical Support System – Medications for Alcohol Use Disorder (PCSS-MAUD)
The Curbsiders Addiction Medicine are proud to partner with Providers Clinical Support System – Medications for Alcohol Use Disorder (PCSS-MAUD) to bring you this episode. PCSS-MAUD is a national project funded by the Substance Abuse and Mental Health Services Administration to provide free, comprehensive training, guidance, and mentoring on the prevention, diagnosis, and treatment of alcohol use disorder (AUD). PCSS-MAUD aims to enhance the capacity of all healthcare professionals to treat individuals with alcohol use disorder, including the use of Food and Drug Administration-approved MAUD. Learn more at www.pcss-maud.org.
Show Segments
- Intro, disclaimer, guest bio
- 4:02 Guest one-liner
- 8:07 Case from Kashlak
- 9:55 Alternate Dosing Strategies for Naltrexone and Acamprosate
- 12:08 Defining successful treatment
- 18:12 Disulfiram
- 32:10 Non-FDA approved MAUD
- 34:35 Topiramate
- 38:05 Gabapentin
- 42:20 Combination therapy
- 43:28 Other Medications
- 48:10 Behavioral Therapy
- 51:05 Take home points
Medications for Alcohol Use Disorder 2.0 Pearls
- There is a menu of evidence-based medications to treat alcohol use disorder (AUD).
- Non-abstinent reductions in drinking are an evidence-based goal for people with alcohol use disorder.
- There is substantive data supporting disulfiram but predominantly with supervised administration in open-label RCTs
- Disulfiram reactions can be thought of as a fast onset and intense hangover that can be severe enough to lead to hospital evaluation.
- Disulfiram is contraindicated in people with unstable cardiac disease due to the risk of a reaction leading to decompensation and in Child-Pugh B/C cirrhosis due to the risk of acute hepatitis,
- Topiramate has substantial supportive data for the treatment of AUD but is limited by side effects and slow titration.
- Gabapentin has the most supportive data in people with AUD and symptoms of alcohol withdrawal.
- Combination therapy with multiple forms of MAUD is generally lacking in evidence but can be considered if people aren’t meeting their goals.
- Other medications (e.g., varenicline, GLP-1s, and baclofen) can be considered if they have other indications or if other medication trials have not been successful.
- Evidence-based behavioral therapy improves treatment outcomes when added to MAUD.
Medications for Alcohol Use Disorder 2.0 with Dr Stephen Holt – Notes
MAUD 1.0
Before jumping into the sequel, if you’re interested in the basics of medications for alcohol use disorder (MAUD), namely more detail on the use of naltrexone and acamprosate, which are often considered first-line MAUD (Reus 2018), check out our Addiction Medicine Season 1 episode #4 Wrapping Our Heads Around Alcohol Use Disorder Meds.
Briefly, naltrexone is often considered first-line due to its ease of use as a once daily oral pill or once monthly intramuscular injection, as well as a wealth of data showing a reduction in alcohol use. (McPheeters 2023). It works as an opioid antagonist and reduces cravings for alcohol use. Although there was previously concern about treatment with naltrexone in the setting of liver disease or transaminase elevations, recent data suggest it is safe for treatment in almost all stages of liver disease, including those with alcohol-related cirrhosis (Raibee 2023, Hill 2024, Thompson, 2024). For individuals with decompensated cirrhosis, clinicians should utilize shared decision-making principles with the patient when considering the use of naltrexone (Raibee 2023, Hill 2024, Thompson, 2024).
Acamprosate is often considered the second line for patients who cannot be treated with naltrexone (i.e. on chronic opioids or medications for opioid use disorder). While data for its use is similarly robust (McPheeters 2023), its use may be limited by pill burden as it is prescribed as 2 333 mg pills three times daily. Dosing must be adjusted to renal function, but it is safe for all stages of liver disease.
Alternate Dosing Strategies for Naltrexone and Acamprosate
When 50 mg oral naltrexone is ineffective, in Dr Holt’s expert opinion, a trial of 100mg is reasonable, although it does not have supportive evidence.
For those who are not interested in taking a daily medication and are not interested in a long-acting injectable, targeted naltrexone is an alternative dosing strategy that can be considered. Targeted naltrexone is the use of as-needed naltrexone in the setting of anticipated cravings or triggers. This strategy has been shown to be effective (Kranzler 2011, Santos 2022), although the data are less robust than daily oral or monthly IM dosing. There is more data for targeted nalmefene, another opioid antagonist, but this medication remains unavailable in the US (Mann 2013)
What is successful treatment?
An important step in treating AUD is partnering with your patient to determine their goal. While the society we live in often values abstinence as the ideal goal and often the only outcome that is considered positive, ample data supports the benefit of reductions in alcohol use. Reduction in alcohol use is a sustainable outcome (Witkiewitz 2021) that is associated with reductions in mortality (Roerecke 2013), alcohol-related consequences and mental health symptoms (Witkiewitz 2017), and improved quality of life and physical health (Witkiewitz 2018).
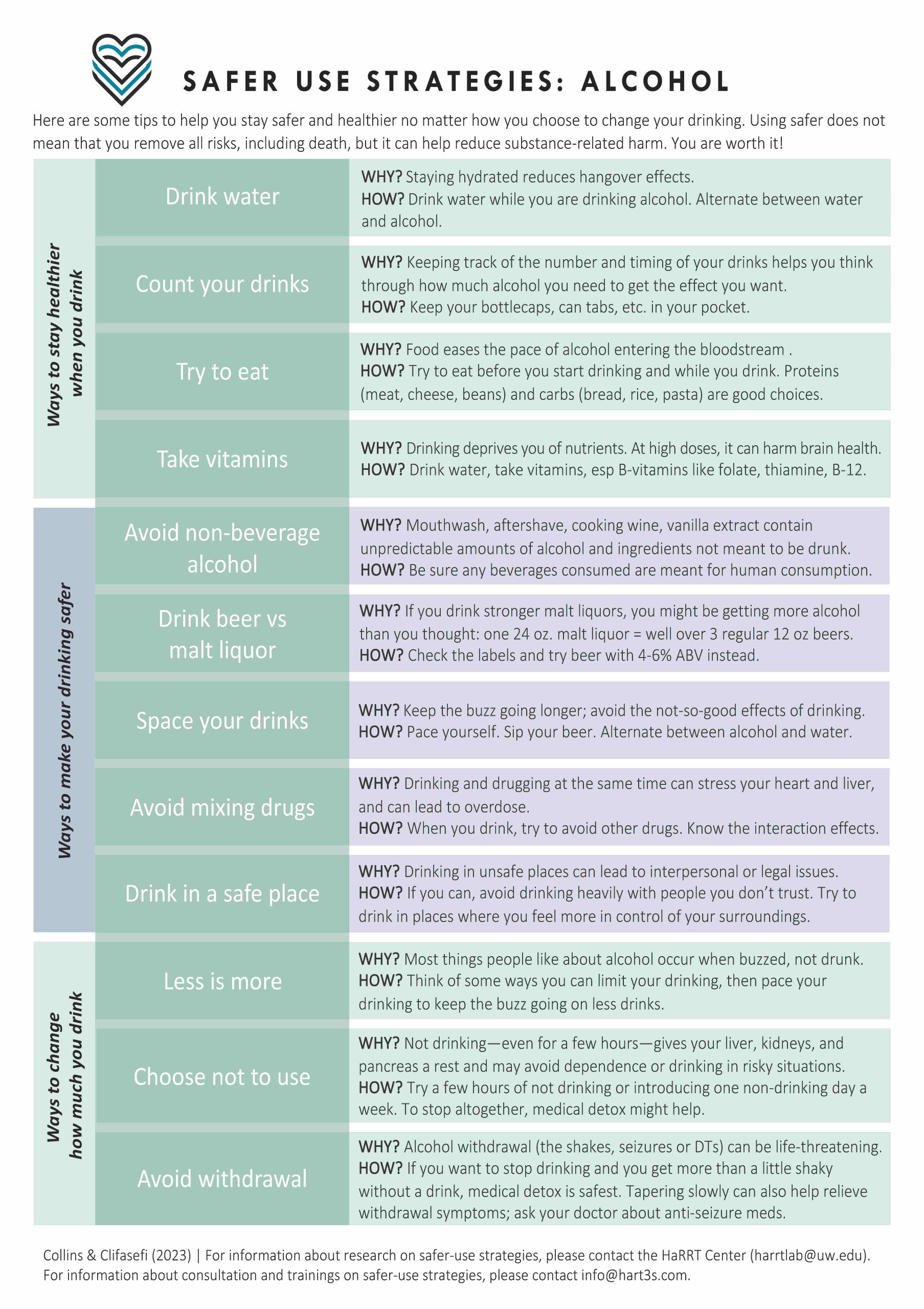
In the setting of continued alcohol use, discussions about safer use and harm reduction are paramount. This can include planning for transportation, ensuring adequate hydration and nutrition, and planning alcohol use to avoid abrupt cessation/reduce withdrawal risk. A great resource from the University of Washington HaRRT Center is available online.
Disulfiram
In Dr Holt’s expert opinion, Disulfiram should be considered as a first line in select situations (Holt 2024), although most guidelines still consider it the second line (Reus 2018, Perry 2022). Disulfiram works as an acetaldehyde dehydrogenase inhibitor, preventing the normal metabolism of alcohol, and causing the buildup of acetaldehyde. This leads to the alcohol disulfiram reaction, which is characterized by flushing, nausea, vomiting, tachycardia, and intense feelings of illness due to acetaldehyde buildup. Disulfiram essentially prevents alcohol use not by reducing cravings but by preventing a person from using alcohol through fear of having an adverse reaction.
Dr Holt explains that there is a misunderstanding of disulfiram in the medical literature that has led to it often not being reasonably considered in AUD treatment. While double-blinded RCTs are the gold standard for most medications, in the case of disulfiram, they are not the appropriate studies to assess efficacy. In a double-blind RCT for disulfiram, the patient would not know whether they have taken disulfiram or placebo and thus, in either arm, would be concerned they may have a reaction if they drink alcohol, thus negating the effectiveness of disulfiram through improving the effectiveness of the placebo. This phenomenon is illustrated in a meta-analysis showing a drastic improvement in alcohol use outcomes in open-label RCTs and no improvement in double-blinded RCTs looking at disulfiram (Skinner 2014).
That being said, disulfiram is most evidence-based when administered under supervision (with a treatment partner observing or reminding the patient to take their medication daily) (Skinner 2014). Disulfiram is also only appropriate if a patient’s goal is complete abstinence. Disulfiram should not be used in patients with cognitive impairment as its efficacy relies on remembering it has been taken and there is a risk of the aversive reaction. In patients at risk of medical or psychiatric (schizophrenia, conditions where they have experienced psychosis) decompensation from a disulfiram reaction, such as those with unstable cardiac disease, disulfiram treatment should be avoided. In general, disulfiram is also avoided in liver disease due to the risk of acute medication-related hepatitis. However, Dr. Holt uses it in patients with up to Child-Pugh A cirrhosis. As these criteria often significantly restrict those eligible for treatment, some argue disulfiram thus remains the second-line treatment for most patients with AUD (Axelrath 2024).
When discussing disulfiram with patients, Dr. Holt emphasizes that he focuses on the impact it can have on someone’s alcohol use and the reduction of negative consequences related to alcohol use to frame the conversation rather than focusing most on the physiologic consequences of drinking when treated with disulfiram. That being said, it is essential to ensure patients understand what a disulfiram reaction feels like before beginning therapy. Additionally, patients should be warned about other alcohol-containing products as well, namely food/sauces made with alcohol and alcohol in mouthwash.
Non-FDA approved forms of MAUD (off-label)
Topiramate
Of the medications non-FDA-approved for AUD, topiramate has the most robust evidence supporting its effectiveness. The data supporting topiramate in the reduction of heavy drinking days, drinks per day, and increasing abstinence is strong enough (Fluyau 2023, McPheeters 2023, Morley 2024) that it is considered co-first line with naltrexone in the most recent VA/DOD guidelines (Perry 2022). Topiramate is also one of the few forms of MAUD that is safe in people with both renal and hepatic impairment, although dose adjustments are necessary.
A marked limitation in the use of topiramate is the burden of side effects, which can include nausea, paresthesias, and changes in taste and are associated with increased medication discontinuation/study dropout (Bahji 2023). Additionally, the effective dose for alcohol use disorder is often 200-300 mg divided into twice-daily doses. Uptitration to that dose in research studies usually takes upward of 8 weeks with weekly dose changes – an intensive process that can be a barrier to treatment uptake.
Gabapentin
Dr. Holt noted a lot of excitement with early data for gabapentin to treat AUD (Mason 2014). However, a subsequent study has shown less consistent benefits (McPheeters 2023), indicating that the benefit may be limited to patients who have experienced alcohol withdrawal. (Anton 2020)
It is worth noting there are other alcohol-associated conditions (i.e. alcohol-induced peripheral neuropathy) where gabapentin may have benefits as well.
Dosing in the research studies often begins at 300 mg TID with subsequent up-titration to 600 mg TID. In Dr Holt’s expert opinion, people with AUD can generally tolerate higher starting doses and faster titration, given the likely cross-tolerance at the GABA receptor between alcohol and GABA-ergic medications like gabapentin.
For an overview of the use of gabapentin in ambulatory alcohol withdrawal (and to learn more about Steve’s love of birding), check out our Addiction Medicine Season 1 episode #2 Get in the Spirit of Ambulatory Alcohol Withdrawal
Gabapentin
Dr. Holt noted a lot of excitement with early data for gabapentin to treat AUD (Mason 2014). However, a subsequent study has shown less consistent benefits (McPheeters 2023), indicating that the benefit may be limited to patients who have experienced alcohol withdrawal. (Anton 2020)
It is worth noting there are other alcohol-associated conditions (i.e. alcohol-induced peripheral neuropathy) where gabapentin may have benefits as well.
Dosing in the research studies often begins at 300 mg TID with subsequent up-titration to 600 mg TID. In Dr Holt’s expert opinion, people with AUD can generally tolerate higher starting doses and faster titration, given the likely cross-tolerance at the GABA receptor between alcohol and GABA-ergic medications like gabapentin.
For an overview of the use of gabapentin in ambulatory alcohol withdrawal (and to learn more about Steve’s love of birding), check out our Addiction Medicine Season 1 episode #2 Get in the Spirit of Ambulatory Alcohol Withdrawal
Other Medication Options
Several other medications have small studies assessing their efficacy. In most cases, these medications can be considered if other, more evidence-based forms of MAUD have not been effective and if there are other indications for their use. They include varenicline, prazosin, and ondansetron (McPheeters 2023).
GLP-1 receptor agonists have gained attention for potential use to treat AUD but still lack any comparative effectiveness data. Therefore, they should only be used if another clinical indication exists (Leggio 2023, Hendershot, 2025).
Baclofen has some supportive but mixed data for its use as MAUD in several recent meta-analyses (McPheeters 2023, Bahji 2023, Agabio 2023). It is often considered in patients with cirrhosis due to an early supportive trial. (Addolorato 2007)
There is no one-size-fits-all approach or single medication that works for all patients. It’s essential to set expectations early that there is a menu of options and that continued follow-up and care through their treatment is critical to finding the treatment plan that works for them.
Other facets of treatment
Behavioral treatment
Evidence-based behavioral treatment should be considered in all patients with AUD and may provide additional benefit to MAUD alone. (Ray 2020) Evidence-based options include cognitive behavioral therapy, motivational enhancement therapy, and Twelve Step Facilitation, all requiring care with a psychologist or therapist. However, behavioral treatment should not be a required part of AUD treatment, given the strong evidence supporting MAUD alone (without behavioral treatment).
Dr Holt mentions that mutual support groups can also be a beneficial adjunct to care particularly as they are easily accessible, free, and provide a supportive community in someone’s recovery journey. Finding a suitable mutual support group can be a key factor in sustaining engagement when additional support is desired. Although Alcoholics Anonymous (AA) is the most widely recognized mutual support groups, there are many other groups with varied focuses. For example, SMART Recovery focuses on CBT, moderation management emphasizes reductions of alcohol use, and Phoenix incorporates physical activity. (SAMHSA 2021).
Whole person care
It’s worth highlighting that the treatment of a person with AUD should work to address the needs of the whole person. Developing a therapeutic relationship and working to understand the reasons for alcohol use (i.e., trauma, untreated anxiety…) and address them is critical!







{kind=link}