
In this post I link to and excerpt from American Society of Hematology 2018 guidelines for management of venous thromboembolism: diagnosis of venous thromboembolism [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Blood Adv. 2018 Nov 27;2(22):3226-3256.
I found the organization of the article difficult to follow. Therefore I just excerpted the flow charts and the recommendations.
For the 2018 guidelines on treatment, please see American Society of Hematology 2018 guidelines for management of venous thromboembolism: optimal management of anticoagulation therapy [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Blood Adv. 2018 Nov 27;2(22):3257-3291.
The flow charts require an estimate of the pretest probability of VTE.
- Wells’ Criteria for Pulmonary Embolism [Link is to MDCalc]
- PERC Rule for Pulmonary Embolism [Link is to MDCalc]
- Wells’ Criteria for DVT [Link is to MDCalc]
Here are the flow charts for the 2018 ASH Guideline on Diagnosis of Venous Thromboembolism:
Low PTP/prevalence (≤ 5%)
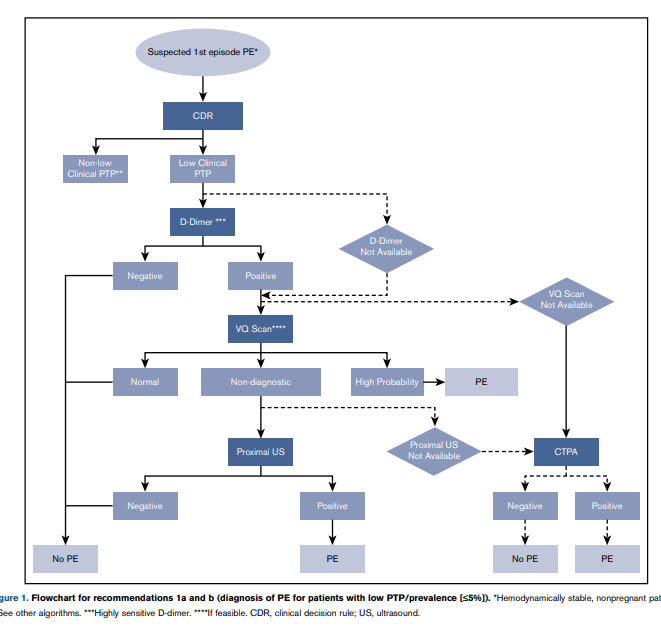
Recommendation 1a
The ASH guideline panel recommends using a strategy starting
with D-dimer for excluding PE in a population with low
prevalence/PTP (</= 5%), followed by VQ scan or CTPA for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing VQ
scan or CTPA alone. (Strong recommendation for D-dimer
based on high certainty in the evidence of effects on clinical
outcomes ÅÅÅÅ and moderate certainty in the evidence of
diagnostic accuracy studies ÅÅÅ◯; conditional recommendation for VQ scan or CTPA based on very low certainty in the evidence of effects on clinical outcomes Å◯◯◯ and low certainty in the evidence from diagnostic accuracy studies ÅÅ◯◯).Recommendation 1b
The ASH guideline panel recommends against using a positive
D-dimer alone to diagnose PE, and against additional testing
following negative CTPA or normal VQ scan in a population with low prevalence/PTP (</= 5%). (See grading for
recommendation 1a.)
Intermediate PTP/prevalence (∼20%)
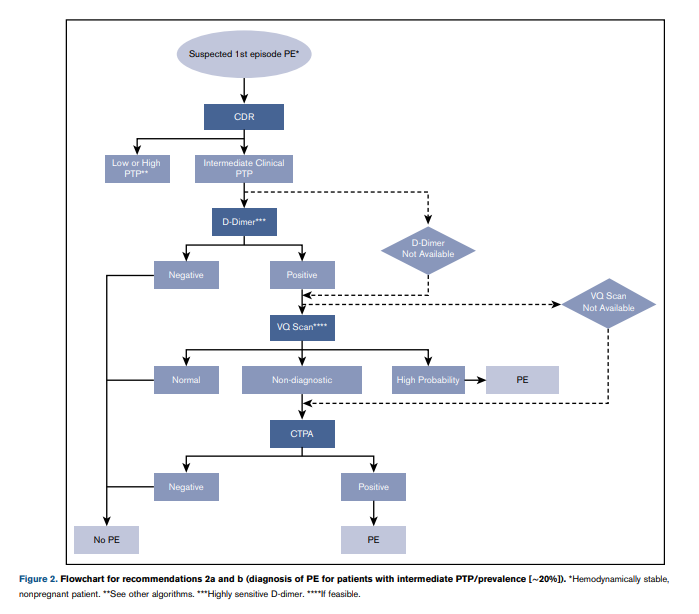
Recommendation 2a
The ASH guideline panel suggests using a strategy starting with
D-dimer for excluding PE in a population with intermediate
prevalence/PTP (∼ 20%), followed by VQ scan or CTPA for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing VQ scan or CTPA alone. Patients who are likely to have a nondiagnostic VQ scan should undergo CTPA. (Conditional recommendation for Ddimer based on high certainty in the evidence of effects on clinical outcomes ÅÅÅÅ and moderate certainty in the evidence about diagnostic accuracy studies ÅÅÅ◯; conditional recommendation for VQ scan or CTPA based on very low certainty in the evidence of effects on clinical outcomes Å◯◯◯ and moderate certainty in the evidence from diagnostic accuracy studies ÅÅÅ◯).Recommendation 2b
The ASH guideline panel recommends against using a positive
D-dimer alone to diagnose PE, and against additional testing
following negative CTPA or normal VQ scan in a population with intermediate prevalence/PTP (;20%). (See grading for recommendation 2a.)
High PTP/prevalence (≥50%)
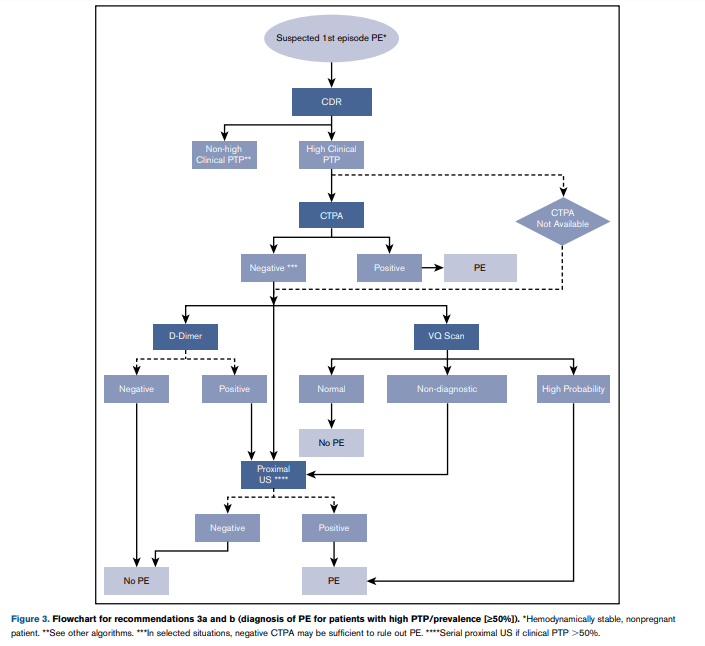
Recommendation 3a
The ASH guideline panel suggests using a strategy starting with
CTPA for assessing patients suspected of having PE in a population with high prevalence/PTP ($50%). (Conditional recommendation for CTPA based on very low certainty in the evidence of effects on clinical outcomes Å◯◯◯ and moderate certainty in the evidence of diagnostic accuracy studies ÅÅÅ◯).
Recurrent PE
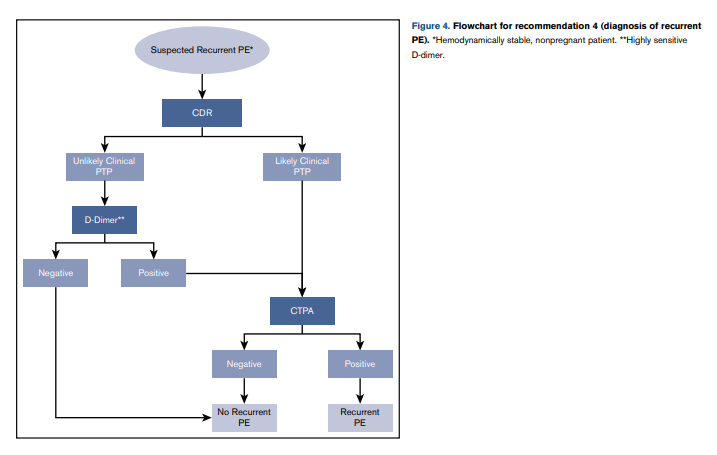
Recommendation 4
The ASH guideline panel suggests using a strategy starting with
D-dimer for excluding recurrent PE in a population with unlikely PTP. Patients with a positive D-dimer or those who have a likely PTP should undergo CTPA. (Conditional recommendation for D-dimer and CTPA based on low certainty in the evidence of effects on clinical outcomes ÅÅ◯◯ and moderate certainty in the evidence from diagnostic accuracy studies ÅÅÅ◯).
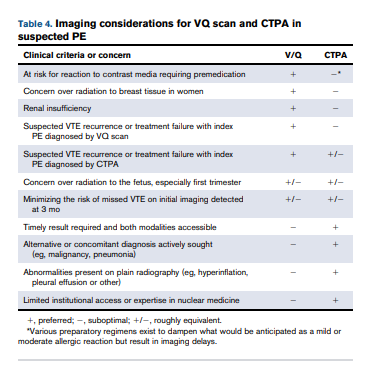
Imaging Considerations For VQ Scan And CTPA in Suspected PE
Diagnosis of lower extremity DVT
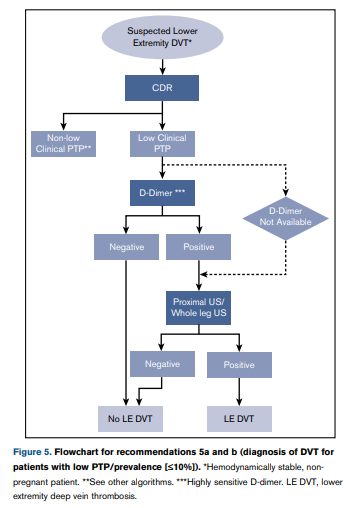
Low PTP/prevalence (≤10%)
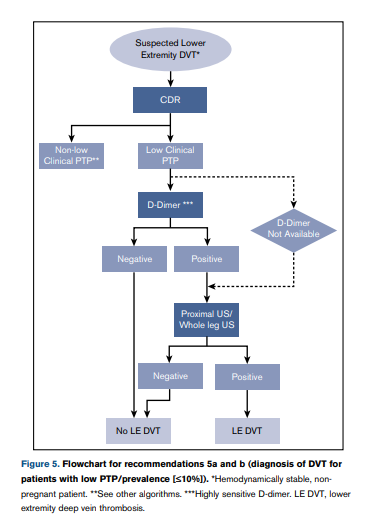
Recommendation 5a
The ASH guideline panel recommends using a strategy
starting with D-dimer for excluding DVT in a population with
low prevalence/PTP (≤ 10%), followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing. If D-dimer is not readily available, alternate acceptable strategies include performing proximal
lower extremity or whole-leg ultrasound alone. (Strong recommendation for D-dimer based on moderate certainty in the evidence of effects on clinical outcomes ÅÅÅ◯ and moderate
certainty in the evidence of diagnostic accuracy studies
ÅÅÅ◯; conditional recommendation for proximal or whole-leg
ultrasound based on very low certainty in the evidence of effects on clinical outcomes Å◯◯◯ and moderate certainty in the
evidence from diagnostic accuracy studies ÅÅÅ◯).Recommendation 5b
The ASH guideline panel recommends against using a positive
D-dimer alone to diagnose DVT, and against additional testing
following negative proximal or whole-leg ultrasound in a population with low prevalence/PTP (#10%). (See grading for
recommendation 5a.)
Intermediate PTP/prevalence (∼25%)
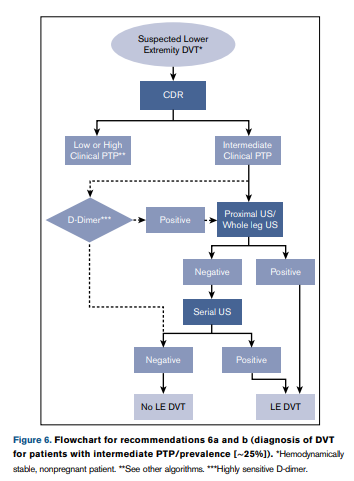
Recommendation 6a The ASH guideline panel suggests using a strategy using whole-leg ultrasound, or starting with proximal lower extremity ultrasound for evaluating patients suspected of
having DVT in a population with intermediate prevalence/
PTP (∼25%). No further testing is required if the whole-leg
ultrasound is negative, but a negative initial proximal ultrasound should be followed by serial proximal ultrasound if no alternative diagnosis is identified.In an intermediate PTP population where the prevalence is lower, other potentially acceptable strategies include proximal lower extremity ultrasound alone with no additional follow-up testing for negative results, or a strategy starting with D-dimer for excluding DVT followed by proximal lower extremity ultrasound or whole-leg ultrasound for patients requiring additional testing. (Conditional recommendation for proximal or whole-leg ultrasound based on very low certainty in the evidence of effects on clinical outcomes Å◯◯◯ and high certainty in the evidence from diagnostic accuracy studies ÅÅÅÅ; conditional recommendation
for D-dimer based on moderate certainty in the evidence of effects
on clinical outcomes ÅÅÅ◯ and moderate certainty in the evidence from diagnostic accuracy studies ÅÅÅ◯)Recommendation 6b
The ASH guideline panel recommends against using a
positive D-dimer alone to diagnose DVT in a population with
intermediate prevalence/PTP (;25%). (See grading for recommendation 6a.)
High PTP/prevalence (≥50%)
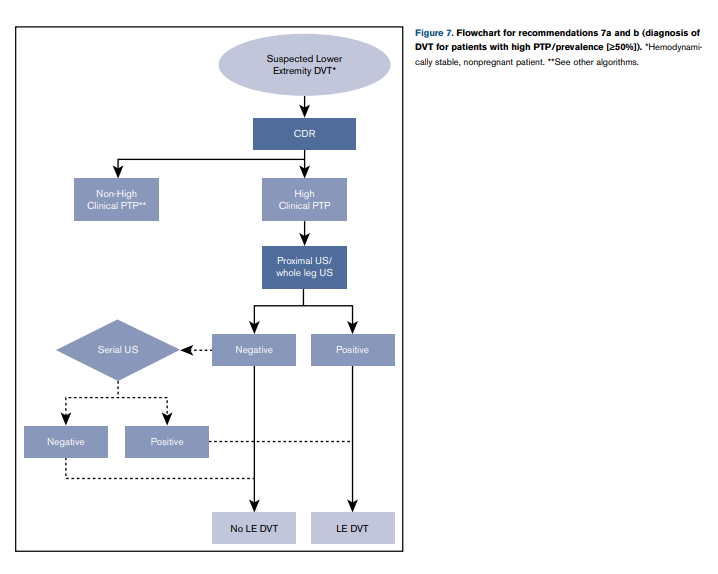
Text for 7a and 7b Start here
Heading for fig8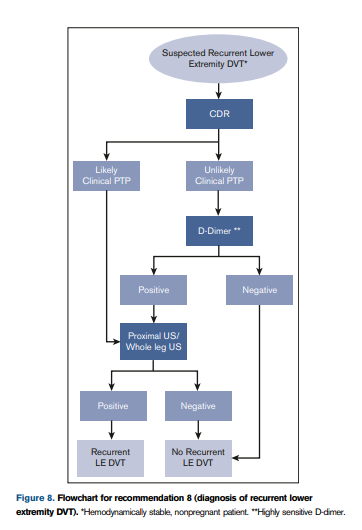

Text

Text
Image



