In this post I link to and excerpt from Brainstem dysfunction in critically ill patients [PubMed Abstract] [Full Text HTML] [Download Full Text PDF]. Crit Care. 2020 Jan 6;24(1):5.
Here are excerpts:
Introduction: the concept of brainstem dysfunction
The brainstem is the caudal portion of the brain that connects the diencephalon to the spinal cord and the cerebellum [1].
The brainstem mediates sensory and motor pathways between the spinal cord and the brain and contains nuclei of the cranial nerves, the ascending reticular activating system (ARAS), and the autonomic nuclei. It controls the brainstem reflexes and the sleep wake cycle and is responsible for the autonomic control
of the cardiocirculatory, respiratory, digestive, and immune systems.Brainstem dysfunction may result from various acute or chronic insults, including stroke, infectious, tumors, inflammatory, and neurodegenerative diseases.
Brainstem dysfunction can then contribute to impairment of consciousness, cardiocirculatory and respiratory failure, and
thus increased mortality [2–5].In the present review, we describe brainstem functional neuroanatomy, clinical syndromes, and assessment methods before addressing the concept of critical illness associated brainstem dysfunction.
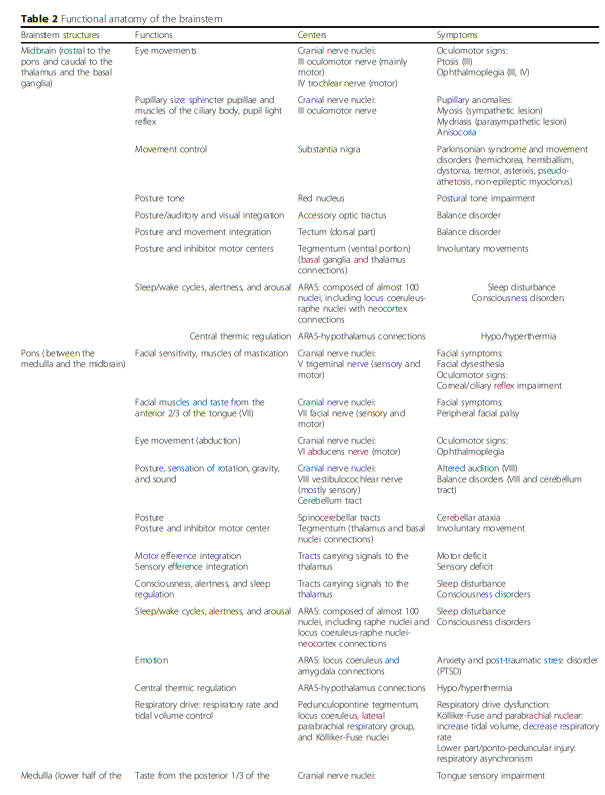
Functional neuroanatomy of the brainstem
The brainstem can be categorized into three major parts: midbrain, pons, and medulla oblongata (Figs. 1 and 2).
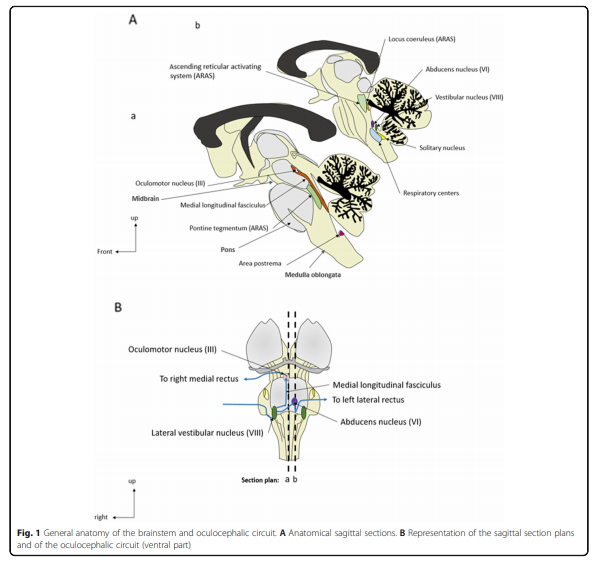
The brainstem contains both gray and white matter, with the basilar artery representing the vascular supply.
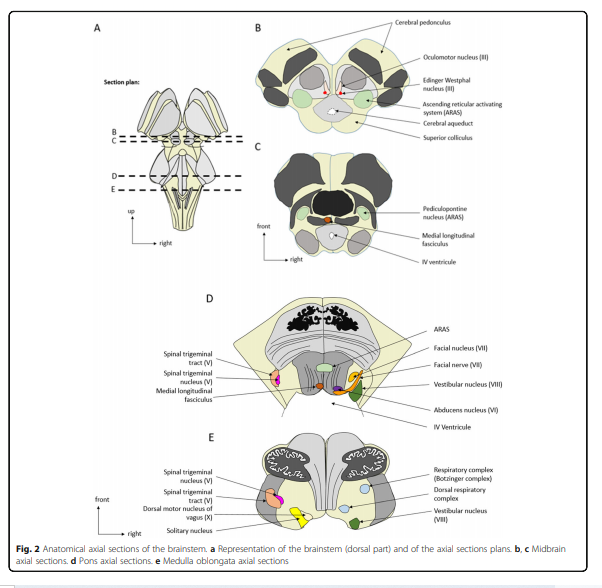
The gray matter includes the nuclei of the cranial nerves
(anterior part), the ARAS (posterior part), the extrapyramidal and the central autonomic nervous system (ANS). This gray matter controls brainstem reflexes, arousal, automatic movements, and homeostasis, respectively.The white matter is composed of ascending sensory pathways and descending pyramidal and extrapyramidal pathways (Table 1).
Brainstem syndromes and assessment
Brainstem pathology should be considered in cases of (a) sensory or motor deficits combined with cranial nerve palsy, (b) impairment of consciousness, (c) dysautonomia, or (d) neurological respiratory failure.
Brainstem motor and sensory deficits and cranial nerve palsy
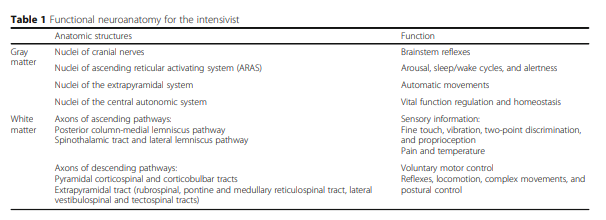
The pyramidal and extrapyramidal tracts connect the upper motor neurons and the extrapyramidal nuclei with the lower motor neurons located in either the brainstem or the spinal cord [6]. While the former controls voluntary movement, the latter is involved in reflexes, motion, complex movements, and postural control (Tables 1 and 2).
Repeating Table 1:
Table 2: